Analysis of the Evolution of Chronic Kidney Disease (CDD) in 960 Diabetic Patients in Mauritania According to Sex, Age and Ethnicity
Author(s): Lella Mohamed Lemine1,3, TFEIL Yahya1,2, Ghaber Sidi Mohamed1,2*, Dahiya Mohamed1,3, Ould El Kebir MV1
1Nutrition, Metabolic Disorders, and Nutrition Research Unit FST University of Nouakchott, Mauritania.
2Faculty of Medicine University of Nouakchott.
3Department of Diabetology and Endocrinology, National Hospital of Nouakchott, Mauritania.
*Correspondence:
Ghaber SM, Unité de Recherche Alimentation, Nutrition et Troubles métaboliques - FST -Université de Nouakchott, Mauritanie.
Received: 30 Jan 2024 Accepted: 07 Mar 2024
Citation: Lella Mohamed Lemine, Yahya T, Ghaber SM, et al. Analysis of the Evolution of Chronic Kidney Disease (CDD) in 960 Diabetic Patients in Mauritania According to Sex, Age and Ethnicity. Diabetes Complications. 2024; 8(1); 1-6.
Abstract
This study sheds light on the progression of CKD (Chronic Kidney Disease) among diabetic patients in Mauritania, providing crucial insights for enhancing prevention, management, and tailoring care for this population. Of the 960 diabetics included in the study, only 26.67% exhibit normal kidney function, while 73.33% have CKD at various stages. Stage 1, termed as "Mild Kidney Insufficiency," is the most prevalent, accounting for 77.13% of all CKD cases. In contrast, stage 4, or "Terminal CKD," affects only 0.28% of the participants.
Looking at the gender distribution, it appears that CKD is slightly more common among male diabetics (40.20%) than among females (31.12%), especially at stage 1 or mild kidney insufficiency. In terms of age distribution, diabetics aged 41 to 70 years old are the most affected by CKD, with a peak between 51 and 60 years for men and between 41 and 50 years for women. Following these peaks, which result from a gradual increase, the prevalence of CKD tends to decrease. Regarding ethnic affiliation, significant disparities arise between the Moors and the Black Africans. Among the men, 89.12% of the Moors suffer from CKD compared to 10.88% of Black Africans. For women, these percentages stand at 89.4% for the Moors and 15.09% for the Black Africans. The stage of mild kidney insufficiency is overwhelmingly the most prevalent, both among the Moors and the Black Africans, affecting 71.24% and 61.01% of men respectively, and 10.10% and 11.01% of women.
Keywords
Introduction
Chronic Kidney Disease (CKD) is a steadily growing global public health issue, affecting millions of individuals worldwide. According to the National Kidney Foundation [1], CKD currently impacts around 10% of the global population, with its prevalence continuing to rise. Among the major risk factors for CKD, diabetes mellitus stands out prominently. Several studies and systematic reviews have confirmed the significant association between diabetes and the onset of CKD [2,3]. The underlying mechanisms of this association are intricate, involving damage to the small blood vessels of the kidneys, inflammation, high blood pressure, and metabolic changes [4,5].
The influence of age on CKD in diabetic patients is a well- documented research topic. Aging is a well-known risk factor for CKD, and it is established that renal function naturally tends to decline with age [6]. Differences in gender concerning the incidence and progression of CKD have also been extensively studied. Epidemiological studies have shown that men and women may have distinct risk profiles in relation to CKD [7]. For instance, a relatively recent meta-analysis revealed that diabetic men have a higher risk of developing CKD compared to diabetic women [8]. Regarding ethnicity, several studies have highlighted significant disparities in the incidence of CKD among diabetic patients from various ethnic groups [9]. For instance, some ethnic populations might exhibit higher rates of CKD, while others might be more susceptible to advanced stages of the disease [10].
The aim of this study was to explore the relationships between diabetes and the progression of Chronic Kidney Disease (CKD), considering sociodemographic factors such as gender, age, and ethnicity. By systematically analyzing these factors, we hope to contribute to a better understanding of the mechanisms underlying this complex association and, ultimately, improve the clinical management of patients with diabetes and CKD. The results of this in-depth analysis may also hold significant implications for personalized medicine and healthcare management in this high- risk population.
Methods
Study Population: Our sample consisted of 960 diabetic patients monitored by the Maurilab Institute in Nouakchott (a specialized medical biology laboratory), of which 532 were men (55.4%) and 428 were women (44.6%).
Measurement of CKD Progression
We assessed the progression of CKD by calculating the creatinine clearance (eGFR in ml/min/1.73m²) within our study population. This analysis allowed us to classify CKD into five distinct stages, ranging from "Normal Stage" to "End-stage CKD", using standard CKD classification criteria.
Statistical Analyses To investigate the relationships between diabetes, CKD progression, and sociodemographic factors, we conducted appropriate statistical analyses using the SPSS software version 25. We employed cross- tabulations to analyze the distribution of diabetic participants based on CKD stage, gender, age, and ethnicity. Percentages were calculated for each category, facilitating the visualization of trends and disparities.
Validation of Results
The results underwent statistical validation, especially through the chi-square test, to determine the statistical significance of observed differences between groups. Significance thresholds were set at a p < 0.05 level.
Research Ethics
This study adhered to the ethical principles governing health science research. All data were collected anonymously, and informed consent was obtained from each participant. The study was previously approved by the Ethics Committee of the University of Nouakchott.
Limitations of the Study
It's worth noting that this study has certain limitations, including the retrospective nature of the data, the possibility of selection bias, and the need to consider other potential risk factors that were not included in this analysis.
Results
Distribution of diabetics based on the stage of chronic kidney disease (CKD) and their gender
Among the 960 diabetics included in the study, only 256 individuals (146 men and 110 women), representing 26.67% of the study population, have normal conditions. The remaining 704 people, or 73.33% of the study population, suffer from CKD (Chronic Kidney Disease) at various stages (Table 1).
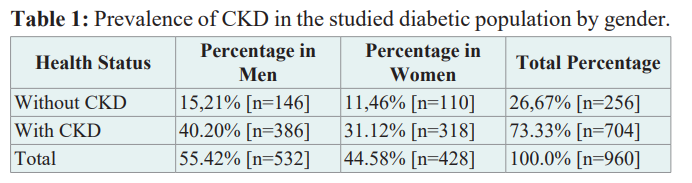
Table 2 indicates that the "Mild Renal Insufficiency" stage is the most common, accounting for 77.13% of all individuals with CKD. On the other hand, the "End-stage CKD" is the least prevalent, with only 2 individuals, making up 0.28% of all CKD cases. Furthermore, this table shows that the number of men is higher than that of women in the "Mild Renal Insufficiency" stage, but it's slightly lower in the other CKD stages. For instance, in the "Mild Renal Insufficiency" stage, there are 314 men compared to 229 women, whereas in the moderate stage, there are 66 men versus 80 women. The severe and terminal stages account for a small portion, not exceeding 2% for the former and 0.5% for the latter among all individuals with CKD.
Distribution of diabetic men based on their age group and the stage of chronic kidney disease (CKD).
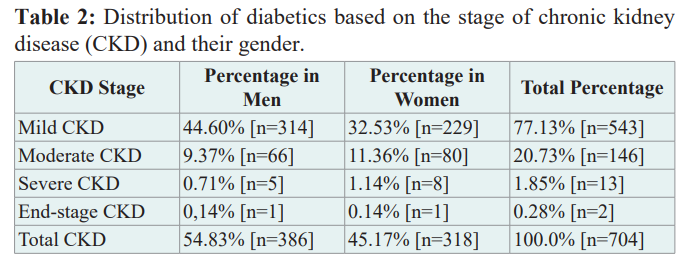
For diabetic men, Table 3 highlights that CKD is most prevalent in the age group of 51 to 60 years, accounting for 147 individuals (38.08% of all observed CKD cases), followed by the age groups of 41 to 50 years and 61 to 70 years, with 77 (19.94%) and 85 individuals (22.02%) respectively. Additionally, the age brackets of 0 to 20 years, 21 to 30 years, and those over 80 years exhibit the lowest rates of CKD, with respective percentages of 0.0%, 1.04%, and 3.62%. Trends by age and CKD stage indicate that the prevalence of CKD among diabetic men gradually increases with age up to 60 years, then progressively declines thereafter. The "Mild Renal Insufficiency" stage is the most frequent across all age groups. The "Moderate CKD" stage is most prevalent in the age groups of 51 to 60 years and 61 to 70 years simultaneously.
Distribution of diabetic women based on their age group and stage of chronic kidney disease (CKD).
Of the 318 women diagnosed with CKD, the age group of greatest concern in terms of CKD is 51 to 60 years, where 110 individuals are observed (34.59% of the total CKD cases among women). This group has the highest rates of mild and moderate CKD, followed by the 41 to 50 years and 61 to 70 years age groups, with 65 individuals (20.44%) each. On the other hand, the age groups of 0 to 30 years and over 80 years have the lowest CKD rates, accounting for 2.51% and 2.83% respectively (Table 4).
Trends by age and CKD stage show that the prevalence of CKD among diabetic women increases progressively with age up to 60 years, and then gradually decreases thereafter. The "Mild kidney failure" stage is the most common in all age groups, except for the 70-80 years group where the "Moderate CKD" stage is more prevalent. The highest rate is observed between 51 and 60 years for the former and between 61 and 70 years for the latter.
Distribution of diabetic patients based on the stage of Chronic Kidney Disease (CKD) and their ethnicity
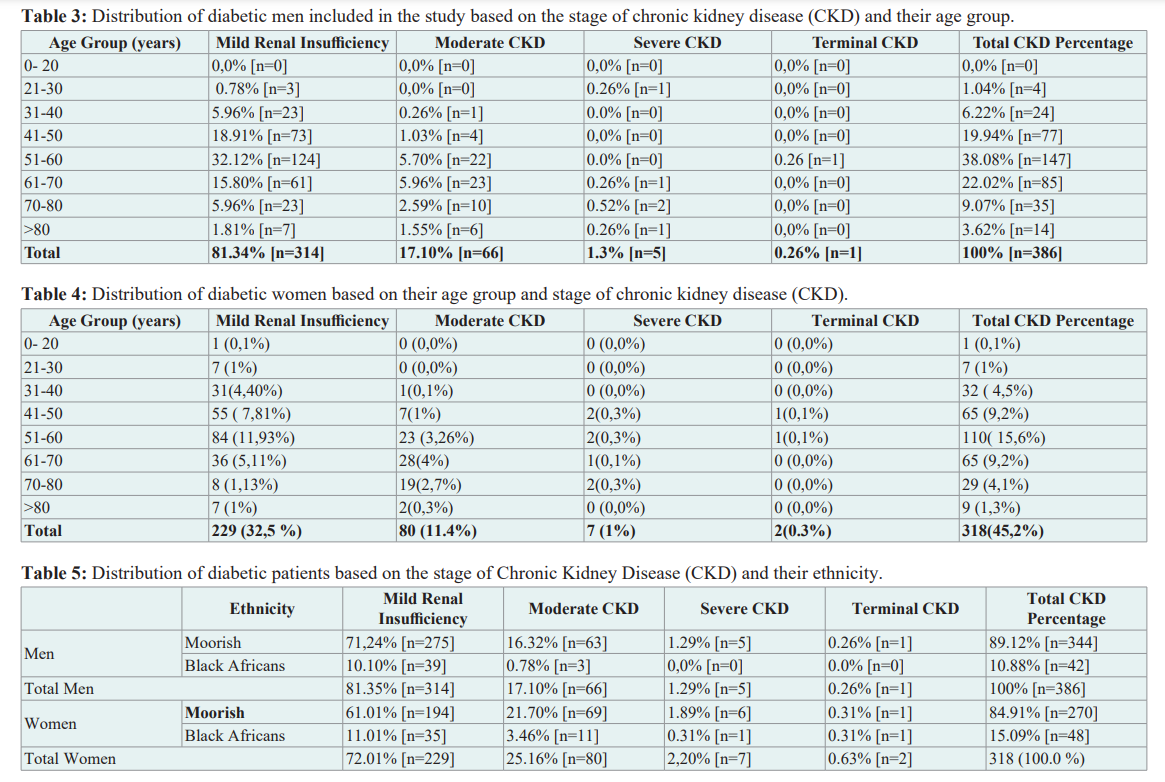
Table 5 highlights significant differences in the prevalence of CKD between the Moorish and Black African ethnic groups among diabetics. The Moors show higher rates of CKD (89.12% in men and 84.91% in women) compared to Black Africans (10.88% in men and 15.09% in women). Among all stages of CKD, stage 1 is the most prevalent in both genders, primarily among the Moors, accounting for 71.24% of all CKD cases in men and 61.01% of CKD cases in women. For Black Africans, these rates are 10.10% and 11.01% for each group, respectively. The "Moderate CKD" stage is also more common among the Moors than among the Black Africans, with rates of 16.32% in men and 21.70% in women, respectively.
Discussions
Distribution of Diabetics by Stage of Chronic Kidney Disease (CKD) and Gender
The close association between diabetes and kidney disease is well- documented in medical literature [11]. However, the observation that the prevalence of chronic kidney disease (CKD) among diabetics in Mauritania stands at 73.33% is both remarkable and concerning. This prevalence might exceed global averages for diabetics [12]. It raises questions about potential gaps in medical care, public health awareness, or management of diabetes and its complications in this specific setting. Our findings also reveal that stage 1 of CKD, often termed "mild kidney failure," is the most prevalent, accounting for 77.13% of all CKD cases. Moderate kidney failure also constitutes a significant proportion, being 20.73% of the total CKD cases.
This observation aligns with prior studies, which have also indicated that early kidney failure is common among diabetic patients [13,14]. This high prevalence aligns with the National Kidney Foundation (NKF) recommendations, which underscore the importance of regular monitoring of kidney function in diabetics, even in the absence of overt symptoms. Studies have shown that early CKD detection and proper management, including blood sugar and blood pressure control, can slow its progression to more advanced stages [15,16]. On the other hand, stage 4, termed "end-stage CKD," and stage 3, termed "severe CKD," account for only 0.28% and 1.85% of all CKD cases, respectively. Though these stages are less frequent, they remain a major concern due to their significant impact on patients' quality of life and their association with elevated mortality rates [17,18]. Patients with end-stage CKD typically require renal dialysis or transplantation, posing a significant burden on the healthcare system. Additionally, the data analysis reveals an interesting trend concerning gender distribution across CKD stages. Overall, men exhibit a slightly higher CKD prevalence than women, though percentages might vary from one stage to another. For instance, in the "mild kidney failure" stage, prevalence in men stands at 44.60% compared to 32.53% in women.
This gender disparity in prevalence might be linked to hormonal, genetic, or behavioral factors influencing CKD progression [19,20]. Previous studies have also reported gender-based prevalence variations in CKD among diabetic patients, though the underlying mechanisms remain not fully understood [21,22].
Distribution of Diabetics by Age Group and Stage of Chronic Kidney Disease (CKD)
The study reveals significant trends in the distribution of diabetics based on their age group and the stage of chronic kidney disease (CKD) that warrant particular attention. The significant increase in CKD prevalence with age among diabetics is a finding solidly supported in the medical literature. This trend is consistent with results from studies like the one conducted by Fox et al. [23], which highlighted a marked correlation between age and the risk of developing CKD in diabetic patients. These findings are also corroborated by a study carried out by Shaw et al. [24]. The older age groups, especially the 51 to 60 years bracket, stand out with notably higher rates of moderate CKD, as well as the presence of a few cases of severe and end-stage CKD. This observation could be attributed to prolonged exposure to diabetes, the accumulation of risk factors, and years of disease management. Studies, such as the one conducted by Afkarian et al. [25], have confirmed that the duration of diabetes is a major risk factor for CKD among diabetics.
On the other hand, the young (0-20 years) and advanced (over 80 years) age groups exhibit extremely low rates of CKD. In the case of the young, this is explained by the fact that CKD is a progressively developing disease and requires time to evolve. Young diabetic men and women have fewer years of exposure to diabetes, explaining their lower CKD rates. As for the advanced age groups, this might be attributed to the possibility that very elderly individuals may have higher mortality from other health issues before CKD can progress significantly. This observation underscores the importance of conducting individualized risk assessments in older individuals with diabetes.
Distribution of Diabetics by Stage of Chronic Kidney Disease (CKD) and Ethnicity
The observation of significant differences in the prevalence of chronic kidney disease (CKD) between the Moorish and Black African ethnic groups, both in diabetic men and women, represents a clinically significant finding that warrants detailed analysis and considerations for renal health management within these diverse populations. This disparity might be attributed to a combination of complex factors, including genetic differences, lifestyle habits, environmental factors, and socio-economic factors. Genetics play a pivotal role in predisposing individuals to CKD, and past studies have identified specific genetic variants associated with an increased risk of CKD in certain ethnic populations [26]. These genetic factors might contribute to the observed disparity. However, it's important to note that the prevalence of CKD is not solely reliant on genetic factors. Differences in lifestyle habits, such as diet, physical activity, and diabetes management, can also influence renal health in men and women. Moreover, environmental factors, such as access to healthcare and screening services, as well as socio-economic conditions, can play a significant role in the prevalence of CKD [27].
The analysis of the distribution of diabetic women based on the stage of chronic kidney disease (CKD) and their ethnicity reveals significant disparities in CKD prevalence between the Moorish and Black African ethnic groups, mirroring those seen in diabetic men. However, the differences become more pronounced when examining the more advanced stages of CKD. The "Mild Renal Insufficiency" stage is the most common in both ethnic groups but is noticeably more prevalent among Moorish ethnic women, accounting for 61.01% of cases, compared to Black African ethnic women, who show only 11.01% of cases, a trend similar to that observed in diabetic men. Similarly, the "Moderate CKD" stage is also more frequent among Moorish ethnic women, reflecting a likeness with male findings.
Conclusions
The alarming prevalence of 73.33% of chronic kidney disease (CKD) among diabetics in Mauritania presents a significant public health challenge for the country. This situation might be indicative of shortcomings in health awareness, medical infrastructure, and the management of diabetes-related complications. Several pressing questions arise: Is this a result of an under-equipped health system, barriers to accessing care, or intrinsic factors specific to Mauritania, whether they be genetic, cultural, or socio-economic?
Concrete steps are imperative to directly address this issue:
- Identifying the underlying causes of this high prevalence is a priority. Socio-economic factors such as access to care and the cost of medications could play a significant role in this scenario.
- Enhanced awareness of the risks of uncontrolled diabetes is It is crucial to initiate educational campaigns to prevent and manage the progression of CKD among the diabetic population.
- The government and health organizations must intensify their efforts to strengthen the medical infrastructure, fund targeted research, and improve the overall management of diabetes and its complications.
- Early detection of CKD, even in the absence of overt symptoms, is of utmost importance, especially since mild renal insufficiency is commonly observed among Mauritanian
- While advanced stages of CKD might be less frequent, they remain critical given their profound impact on patients' quality of life and the associated high costs.
- The observed ethnic disparities in CKD prevalence underscore the need to tailor care based on ethnic specificities, including heightened monitoring for higher-risk ethnic groups.
- It is essential to adapt CKD management strategies based on patients' ethnic backgrounds, ensuring timely and tailored interventions for each group.
- Lastly, in-depth studies are required to untangle the various factors, be they genetic, environmental, or social, contributing to these ethnic disparities in Mauritania. A more profound understanding of these elements would help refine preventive and curative strategies for the country's diabetic population.
In summary, given the high prevalence of CKD among diabetics in Mauritania, a multi-sectoral, comprehensive, and tailored approach is needed to provide effective and sustainable solutions to this public health issue.
Competing interests
The authors declare that they have no competing interests.
Author contributions
All authors contributed to the conduct of this work. All authors also declare that they have read and approved the final version of the manuscript.
References
- Kidney Disease Improving Global Outcomes Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Kidney International Supplements. 2021; 11: e142-e163.
- Deshpande AD, Harris Hayes M, Schootman M, et al. Epidemiology of Diabetes and Diabetes Related Complications. Physical Therapy. 2016; 96: 1558-1567.
- Afkarian M, Sachs MC, Kestenbaum B, et Kidney disease and increased mortality risk in type 2 diabetes. Journal of the American Society of Nephrology. 2016; 28: 353-362.
- Brenner BM, Cooper ME, de Zeeuw D, et al. Effects of Losartan on Renal and Cardiovascular Outcomes in Patients with Type 2 Diabetes and New England Journal of Medicine. 2001; 345: 861-869.
- Thomas MC, Cooper ME, Zimmet P, et Changing Epidemiology of Type 2 Diabetes Mellitus and Associated Chronic Kidney Disease. Nature Reviews Nephrology. 2015; 12: 73-81.
- Glassock RJ, Rule AD. The International Kidney Disease Improving Global Outcomes Consortium the implications of anatomical and functional changes of the aging kidney with an emphasis on the Kidney International. 2012; 82: 270-277.
- Huang Y, Cai X, Mai W, et Association Between Prediabetes and Risk of All cause Mortality and Cardiovascular Disease Updated Meta Analysis. BMJ. 2020; 370: m2297.
- Xu Y, Wang L, He J, et Prevalence and Control of Diabetes in Chinese Adults. JAMA. 2017; 317: 2515-2516.
- Kramer HJ, Nguyen QD, Curhan G, et Renal Insufficiency in the Absence of Albuminuria and Retinopathy Among Adults with Type 2 Diabetes Mellitus. JAMA. 2008; 299: 2857-2864.
- Crews DC, Charles RF, Evans MK, et al. Poverty race and CKD in a racially and socioeconomically diverse urban population. American Journal of Kidney Diseases. 2014; 64: 478-485.
- Zimmet Global epidemiology of diabetes mellitus and its complications. Nature Reviews Endocrinology. 2016.
- Cho NH. IDF Diabetes Atlas Global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Research and Clinical Practice. 2018.
- Levey AS, Becker C. Diabetes and nephropathy new insights into the natural history of diabetic kidney disease. Kidney International. 1995; 47: 9-19.
- De Boer IH, Rue Hall YL, et al. Common infections in diabetes pathogenesis management and relationship to glycaemic control. Diabetes Vascular Disease Research. 2011; 8: 95-104.
- Tuttle KR, Bakris GL, Bilous RW, et al. Diabetic kidney disease a report from an ADA Consensus Conference. American Journal of Kidney Diseases. 2014; 64: 510-533.
- Zoungas S, Woodward M, Li Q, et al. Impact of age age at diagnosis and duration of diabetes on the risk of macrovascular and microvascular complications and death in type 2 Diabetologia. 2014; 57: 2455-2464.
- Saran R, Robinson B, Abbott KC, et US Renal Data System 2016 Annual Data Report Epidemiology of Kidney Disease in the United States. American Journal of Kidney Diseases. 2017; 69: A7-A8.
- Tonelli M, Wiebe N, Knoll G, et Systematic review kidney transplantation compared with dialysis in clinically relevant outcomes. American Journal of Transplantation. 2011; 11: 2093-2109.
- Neugarten J, Golestaneh L. Gender and the prevalence and progression of renal disease. Advances in Chronic Kidney Disease. 2013; 20: 390-395.
- Naderi N, Kleine CE, Park C, et Racial and socioeconomic disparities in kidney transplantation. Transplantation Reviews. 2013; 27: 43-49.
- Neugarten J, Acharya A, Silbiger SR, et Gender differences in end stage renal disease. American Journal of Kidney Diseases. 2000; 36: 737-744.
- Jha V, Garcia Garcia G, Iseki K, et Chronic kidney disease global dimension and perspectives. The Lancet. 2013; 382: 12-16.
- Fox CS, Matsushita K, Woodward M, et al. Associations of kidney disease measures with mortality and end stage renal disease in individuals with and without diabetes a meta analysis. The Lancet. 2016; 380: 1662-1673.
- Shaw JE, Sicree RA, Zimmet PZ, et Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes research and clinical practice. 2010; 87: 4-14.
- Afkarian M, Zelnick LR, Hall YN, et al. Clinical Manifestations of Kidney Disease Among US Adults With JAMA. 2016; 316: 602-610.
- Parsa A, Kao WH, Xie D, et APOL1 risk variants race and progression of chronic kidney disease. New England Journal of Medicine. 2013; 369: 2183-2196.
- Crews DC, Bello AK, Saadi G, et World Kidney Day 2014 Increasing Awareness of Chronic Kidney Disease and Aging. Kidney International. 2014; 85: 257-259.