Breast Cancer Patterns and Surgical Oncology Practice in a Low-Income Setting of Sub-Saharan Africa
Author'(s): Ulrich Igor Mbessoh Kengne1*, Jaafar Ibn Abou TalibThiam1, Mamadou Ndiaye1, Salif Balde1, Amacoumba Fall1, Esaie Kasokota1, Awa Niasse1, Mamadou Sow1, Mohammed Ezzet Charfi1 and Sidy Ka1,2
1Oncology department of Dalal Jamm University Hospital, Dakar, Senegal.
2 2Department of Surgery and Specialties, Faculty of Medecine, Pharmacy and Odontostomatology, Cheikh Anta Diop University, Dakar, Senegal.
*Correspondence:
Ulrich Igor Mbessoh Kengne, Oncology department of Dalal Jamm University Hospital, Dakar, Senegal.
Received: 20 Feb 2024; Accepted: 22 Mar 2024; Published: 31 Mar 2024
Citation::: Ulrich Igor Mbessoh Kengne, Jaafar Ibn Abou TalibThiam, Mamadou Ndiaye, et al. Breast Cancer Patterns and Surgical Oncology Practice in a Low-Income Setting of Sub-Saharan Africa. Cancer Sci Res. 2024; 7(1): 1-4
Received: 20 Feb 2024; Accepted: 22 Mar 2024; Published: 31 Mar 2024
Citation:: Ulrich Igor Mbessoh Kengne, Jaafar Ibn Abou TalibThiam, Mamadou Ndiaye, et al. Breast Cancer Patterns and Surgical Oncology Practice in a Low-Income Setting of Sub-Saharan Africa. Cancer Sci Res. 2024; 7(1): 1-4.
Abstract
Objective: The purpose of the study was to highlight epidemiological and clinical specificities of BC in our setting as well as surgical management approaches.
Methods: A retrospective cross-sectional study was conducted in the surgical oncology unit of the Dalal Jamm University Hospital from January to July 2023. Dalal Jamm University Hospital is a teaching hospital based in Dakar, Senegal.
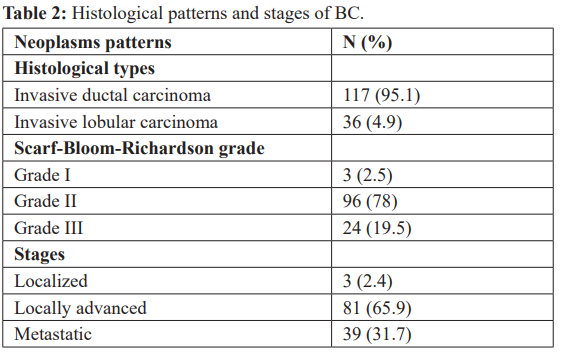
Results: The median age for BC was 45 years (37-54). The main histological types of BC were invasive ductal carcinoma (IDC) and invasive lobular carcinoma (ILC) with respectively 95.1% and 4.9% of cases. SBR grades 2 and 3 were more common with respectively 78% and 19.5% of cases. BC was locally advanced in 65.9% of cases and metastatic in 31.7% of cases. Modified radical mastectomy (MRM) was the main surgical management approach with 97.6% of cases followed by lumpectomy or breast-conserving surgery (BCS) with 2.4% of cases.
Conclusion: The mean age of BC in sub-Saharan African populations is relatively younger than European and American ones. Furthermore, women present with advanced stages of disease explaining higher rate of NAC in African setting than Europe and America. Finally, MRM is the most common surgical management procedure in sub-Saharan Africa whereas it is BCS (lumpectomy) in Europe and America.
Keywords
Introduction
Female breast cancer (BC) is the most frequently diagnosed cancer and the leading cause of cancer mortality in women worldwide [1 3]. In 2020, over 2.3 million patients were newly diagnosed with BC and 685,000 death from breast cancer occurred in 2020 [1]. Breast cancer is recognized as an increasingly important burden of disease, particularly among women in African countries [4]. Among women from Sub-Saharan Africa however, it is second most frequent after cervical cancer [5]. The management of breast cancer is multimodal and this could be very challenging to physicians in the developing countries [6]. The choice of therapy is more often than not dictated by the local availability of resources [6]. The role of surgery for the loco-regional clearance cannot be over-emphasized as it represents the most popular option when there is limited infrastructure and access to chemotherapy and radiotherapy [6]. This study aimed to highlight epidemiological and clinical specificities of BC in our setting as well as surgical management approaches
Materials and Methods
Study Design
A retrospective cross-sectional study was conducted in the surgical oncology unit of the Dalal Jamm University Hospital from January to July 2023. Dalal Jamm University Hospital is a teaching hospital based in Dakar, Senegal. It is the greatest cancer care reference center in the country. The local institutional review board approved this retrospective study, which waived the requirement to obtain written informed consent from patients.
Data Collection
All medical records of patients operated for breast cancer were selected from the archives. Records containing relevant variables for the study were included. Those variables were age, gender, histological type of BC, Scarf-Bloom-Richardson grade, stage and surgical management approach. Medical records missing at least one of these data were systematically excluded from the study. All relevant data were first reported on a questionnaire and then registered in statistical analysis software.
Data Analysis
SPSS statistical software package version 25.0 (Statistical Package for Social Sciences) was used to carry out the statistical analysis of the data. Age of patients was described by median, interquartile range and age groups. Categorical variables were presented by effectives and percentages in frequency tables. Chi-square test was used to look for a potential relationship between the stages of BC and administration of a neoadjuvant chemotherapy as well as the surgical management approach. A p-value less than 0.05 was considered as statistically significant
Results
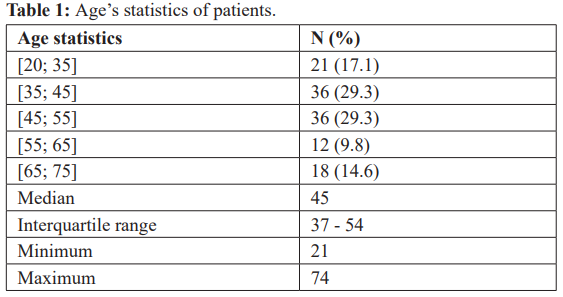
One hundred twenty three patients with BC were included in the study. All patients were females. The median age for BC was 45 years and 46.4% of females were under 45 years old (see Table 1)
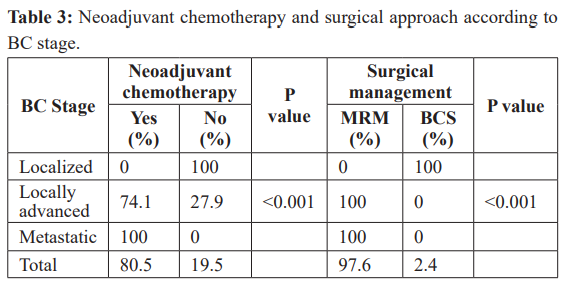
A neoadjuvant chemotherapy was administered in 80.5% of patients including 74.1% of locally advanced BC and all metastatic BC, whereas no localized BC received neoadjuvant chemotherapy
Discussion
This study has been conducted with the purpose of highlighting epidemiological and clinical specificities of BC in our setting as well as surgical management approaches. Articles published in Africa reveal that females are far more affected by BC than males [3-12]. In agreement with this strong evidence, all patients in this study was females. Note that in males, the breast is a rudimentary structure, relatively insensitive to endocrine influences. Various publications on the topic shows that black African populations present at a relatively younger age compared to white-skinned African populations. Indeed, the mean age of BC in black African populations range from 45 to 48 [4,6-9,11,13]; yet, in white skinned populations, the mean age is around 52 years and tends to be similar to that of European natives [1,2,10,12,14]. This findings highlights an interracial difference in populations at risk for breast cancer. The two major histological types of BC in this study were IDC and ILC with respectively 93.2% and 4.5% of cases. These findings are concordant with those in several publications made in Africa [4-13]. Furthermore, grade 2 and grade 3 were in majority regarding to the Scarf-Bloom-Richardson grade with 78% and 19.5% of cases respectively. Same findings have been reported in many studies [9,12,13]. Unlike Europe and America, women present with advanced stages of BC in Africa [1-3]. This observation is corroborated by this study as well as studies of Ranaivomanana et al. in Madagascar, Okifo et al. in Ghana, Deressa et al. in Ethiopia, Cubasch et al. in South Africa, Fitzpatrick et al. in Senegal and Olaogun et al. in Nigeria [3,4,6-8,14]. For Cubasch et al., reasons of this may be poorer patient awareness, lack of population screening programs, cultural barriers, and poor access to a sometimes dysfunctional health care system [3]. Furthermore, Clegg-Lamptey found that some were due to delays caused by previous medical consultations or ignorance or the painless nature of the lump and the fact that the patients thought the lump might disappear [4]. Additionally, Okifo et al. reported that women in Ghana are likely to resort to traditional or spiritual treatment methods, and when those methods fail, they turn to orthodox medical advice [4]
Unlike in Europe where Heinig et al. reported that the proportion of patients with neoadjuvant systemic therapy (NAC) were ranged 2-12% [2], in this study, a NAC was administered in 80.5% of patients including 74.1% of locally advanced BC and all metastatic BC, whereas no localized BC received neoadjuvant chemotherapy and there was a significant association between advanced stage of disease and administration of NAC
Most studies conducted in African setting revealed that MRM is the most common surgical procedure performed in patients with BC [3,6,8]. In this study, MRM was performed in the large majority (97.6%) of patients whereas BCS (lumpectomy) was performed in 2.4% of cases. Furthermore, Amouzou et al. reported in a meta analysis of surgical procedures for female breast cancer in sub Saharan Africa that the rate of MRM in all studies was superior to 60% [16]. This African observation is however antagonistic to the European one where Heinig et al. reported that BCS was the most common surgical procedure performed [2]. An explanation of this antagonism may be that comparatively to Africa, in Europe most patients present in early stages of BC due to many health access facilities like insurance coverage, efficient screening programs and effective health policies
Conclusion
The mean age of BC in sub-Saharan African populations is relatively younger than European and American ones. Furthermore, women present with advanced stages of disease explaining higher rate of NAC in African setting than Europe and America. Finally, MRM is the most common surgical management procedure in sub-Saharan Africa whereas it is BCS (lumpectomy) in Europe and America.
References
- Kadys A, Gremke N, Schnetter L, et al. Intercontinental comparison of women with breast cancer treated by oncologists in Europe, Asia, and Latin America: a retrospective study of 99,571 patients. J Cancer Res Clin Oncol. 2023; 149: 7319-7326.
- Heinig M, Heinze F, Schwarz S, et al. Initial and ten-year treatment patterns among 11,000 breast cancer patients undergoing breast surgery—an analysis of German claims data. BMC Cancer. 2022; 22: 130.
- Cubasch H, Joffe M, Ruff P, et Breast conservation surgery versus total mastectomy among women with localized breast cancer in Soweto, South Africa. PLoS One. 2017; 12: e0182125.
- Okifo FO, Tuoyire DA, Appiah AB, et al. Breast cancer treatment and outcomes at Cape Coast Teaching Hospital, Ghana. Ghana Med J. 2021; 55: 190-197.
- Ssemmanda S, Katagirya E, Bukirwa P, et Breast diseases histologically diagnosed at a tertiary facility in Uganda (2005–2014). BMC Cancer. 2018; 18: 1285.
- Olaogun JG, Omotayo JA, Ige JT, et al. Socio-demographic, pattern of presentation and management outcome of breast cancer in a semi-urban tertiary health Pan Afr Med
- 2020; 36: 363.
- Fitzpatrick MB, Rendi MH, Kiviat NB, et al. Pathology of Senegalese breast cancers. Pan Afr Med J. 2019; 34: 67.
- Deressa BT, Cihoric N, Badra EV, et al. Breast cancer care in northern Ethiopia – cross-sectional BMC Cancer. 2019; 19: 393.
- Engbang JPN, Essome H, Koh VM, Set al. Cancer du sein au Cameroun, profil histo-épidémiologique: à propos de 3044 cas. Pan Afr Med J. 2015; 21: 242.
- Khalil AI, Bendahhou K, Mestaghanmi H, et Cancer dusein au Maroc: profil phénotypique des tumeurs. Pan Afr Med
- 2016; 25: 74.
- Aka E, Horo A, Koffi A, et [Management of breast cancer in Abidjan: A single center experience]. Gynecol Obstet Fertil Senol. 2021; 49: 684-690.
- Fouhi ME, Benider A, Gaëtan KZA, et al. Profil épidémiologique et anatomopathologique du cancer de sein au CHU Ibn Rochd, Pan Afr Med J. 2020; 37: 41.
- Zingue S, Atenguena EO, Zingue LL, et al. Epidemiological and clinical profile, and survival of patients followed for breast cancer between 2010 and 2015 at the Yaounde General Hospital, Cameroon. Pan Afr Med J. 2021; 39: 182.
- Ranaivomanana M, Hasiniatsy NRE, Rakotomahenina H, et al. Aspects épidémio-cliniques des cancers du sein au Service d´Oncologie de Fianarantsoa, Madagascar de 2011 à 2018. Pan Afr Med J. 2021; 38: 264.
- O’Neil DS, Nietz S, Buccimazza I, et al. Neoadjuvant Chemotherapy Use for Nonmetastatic Breast Cancer at Five Public South African Hospitals and Impact on Time to Initial Cancer Therapy. Oncologist. 2019; 24: 933-44.