Effect of Antisense Oligonucleotides Directed Against BCL-2 on Immunotherapy Markers PD-1, PD-L1 and CDK-12 IN LNCaP Cells - A Human Derived Prostate Cancer Line Likely Susceptible to Immunotherapy is Altered by Treatment
Author'(s): Marvin Rubenstein, PhD1,2,3,*
1 Research Program Administered by the Hektoen Institute for Medicine, U.S.A.
2 Departments of Biochemistry, and 3 Urology, Rush University Medical Center, Chicago, IL.,60612, U.S.A.
*Correspondence:
Marvin Rubenstein, Principle Urology Investigator, Hektoen Institute for Medicine, 1070 Cobblestone Ct., Northbrook, IL 60062, U.S.A, Tel: 847-291-7410.
Received: 17 January 2019; Accepted: 02 February 2019
Citation: Marvin Rubenstein. Effect of Antisense Oligonucleotides Directed Against BCL-2 on Immunotherapy Markers PD-1, PD-L1 and CDK-12 IN LNCaP Cells - A Human Derived Prostate Cancer Line Likely Susceptible to Immunotherapy is Altered by Treatment. Cancer Sci Res. 2019; 2(1); 1-7.
Abstract
Background: Almost 25 years ago we first employed antisense oligonucleotides (oligos) against human derived prostatic LNCaP cells using both in vitro [1] and in vivo [2] models; initially targeting the epidermal growth factor receptor, and its ligand transforming growth factor-alpha. Similar studies and results were found when we treated in vitro and in vivo breast cancer models [3]. Clinically, oligos have been employed to treat cancer patients (including those with prostate tumors), targeting apoptosis inhibitors (bcl-2, clusterin) in attempts to restore tumor chemo- [4] or radio-sensitivity [5].
Yet, in spite of these patient trials and additional advances in early detection of prostate cancer, its treatment has not greatly improved in recent years. In the last few years gene therapy and newly discovered immune checkpoint blockade has given some indication that they could provide some additional improvement, particularly when administered following surgery, chemotherapy or irradiation.
As the role of the immune system in cancer treatment becomes better understood (and embraced), some oligos have been found to alter the immune response towards prostate tumors, in previously un-thought of ways. Using oligos (either mono- or bispecific) targeting bcl-2 we found that certain antisense oligos have secondary conformations based on intra strand sequences which permit complementary base pair binding within the oligo, that can induce interferon [6], enhance cell surface antigen expression [prostate specific membrane antigen (PSMA)] [6], and potentially increase tumor recognition and targeting by the immune system.
However, our studies also indicate that gene therapy employing oligos directed towards bcl-2 (in LNCaP cells) frequently are compensated for by altered regulation of apoptosis, increased androgen sensitivity and enhanced oncogene activity [7-9]. Fusion protein TMPRS22 [10] and fusion transcription protein FLI-1 [11] were also increased. All compensation mechanisms noted here suggest increased proliferation, chromosomal instability and greater mitotic activity, producing a more aggressive tumor, or selection of a subset of such cells. This is confirmed by finding greatly increased expression of proliferation factor KI-67 [11] and mitosis related cyclin D1 [11] after treatment directed at bcl-2.
We now believe that immunologic recognition can be an additional pathway for compensation following suppressive bcl-2 treatment and suggest that this type of gene therapy could also influence proteins associated with immune checkpoint blockade, altering its efficacy. Immune checkpoint blockade therapy has become the “standard of care” treatment for melanoma and is now being evaluated (and sometimes recommended for first line treatment) against kidney, lung, hematologic cancers as well as solid tumors (including those of the prostate). Melanoma has a long history of immunotherapy, first using in vitro cultivated lymphokine activated killer (LAK) T cells and then employing similarly cultivated and expanded tumor infiltrating lymphocytes (TIL). The addition of additional cytokines (or their cellular production) enhanced the technique. More recently melanoma became the first tumor to be extensively treated by monoclonal agents in checkpoint blockade, where it prolonged survival and even produced some cures in a small percentage of patients. Studies are now in progress to identify those patients most susceptible for this treatment (those having greater tumor surface expression of PD-1) and even ways to alter susceptibility through evaluation of the patients colon microbiota (with possible alteration using fecal transplantation).
In a continuation of these studies, and also to see whether compensation has additional effects on the immune response, we found that PD-1 and its ligand PD-L1 were significantly enhanced in their expression following treatment with both mono- and bispecific oligos directed towards bcl-2. Similarly the prognostic indicator cyclin derived kinase-12 (CDK-12), which identifies a subpopulation of prostate tumors susceptible to immunotherapy was similarly enhanced. The lack of CDK-12 expression in untreated LNCaP cells suggests that this human derived tumor would be susceptible to immunotherapy for in vivo studies. The fact that treatment enhanced both the expression of PD-1 and PD-L1 targets, in addition to CDK-12 shows the complexity of immune therapy using checkpoint inhibitors, which is far from understood. The greatly enhanced expression of CDK-12 would suggest that the LNCaP cells would no longer be susceptible to checkpoint inhibition at the PD-1/PD-L1 level even though these proteins (and particularly PD-1) present a better target. The huge increase in CDK-12 found in the treatments groups would probably overwhelm such recognition.
Keywords
Introduction
Antisense oligonucleotides (oligos) have been employed in both in vivo and in vitro prostate cancer models employing LNCaP and PC-3 cell lines [2]. Similar studies have employed the MCF- 7 breast cancer cell line [12]. Clinical trials employing oligos have targeted protein growth factors, androgens, receptors for stimulating factors, inhibitors of apoptosis (bcl-2 and clusterin) and oncogenes. Some (OGX-011 developed by Oncogenex Pharmaceuticals) have been studied in clinical trials while others (OGX-225) reached preclinical development [13]. Oligos act through a variety of mechanisms and provide a specific and relatively non-toxic [14] method for translational arrest by degradation of annealed mRNA: oligo duplexes by RNase H, protein binding, DNA triplex formation and especially DNA-RNA triplex formation [1]. In attempts to increase the efficacy of oligos our lab has been evaluating bispecific derivatives [15] with more than one binding site on a single DNA strand. Bispecifics were developed in order to suppress the expression of two gene products. In LNCaP cells we found that mono-specific oligos targeting bcl- 2 and bispecifics targeting both bcl-2 and the epidermal growth factor receptor (EGFR) have comparable activities in suppressing bcl-2 expression as determined by both in vitro growth and bcl-2 expression [16]. Therefore, the presence of a second binding site does not diminish activity of the other.
In theory gene therapy should be specific and lack non-specific effects. In practice this is not so, and the non-specific effects can compromise the initial attempt to control tumor growth. Since these approaches are now in clinical practice, and new trials are constantly being initiated, the recognition of side effects is increasingly important to enhance efficacy of this innovative therapy. In the LNCaP model, cells treated with mono- or bispecific oligos targeting bcl-2 were extracted for RNA and evaluated for protein expression employing RT-PCR. In addition to the compensatory mechanisms already mentioned, some of our more notable findings were the inhibition of bcl-2 with antisense oligos suppressed the apoptotic promoter caspase-3 [17] in an attempt to restore apoptosis following bcl-2 suppression; and enhanced androgen sensitivity via increased expression of the androgen receptor (AR), and AR variants ARv7 and ARv9 [18]; AR co-activators p300, interleukin-6 (IL-6); oncogene viral myelocytomatosis (v-MYC) [19]; and signal transducer and activator of transcription3 (STAT3) proteins [20]. This suggested that following bcl-2 suppressive therapy, there could be selective pressure for a more rapidly growing aggressive (androgen- sensitive, oncogene driven) phenotype, as suggested following the discovery of enhanced expression of both KI-67 (a proliferation marker) and cyclin D1 (a regulator of mitosis). Recognition of this transition is important if either gene therapy or immune checkpoint blockade were to be employed.
Immune checkpoint blockade therapy has become the “standard of care” treatment for melanoma and is now being evaluated for kidney, lung, hematologic cancers as well as solid tumors (including those of the prostate). Melanoma has a long history of attempts at immunotherapy first using lymphokine activated killer (LAK) T cells, later with more potent tumor infiltrating lymphocytes (TIL). Proliferation (in vitro) and overall potency of these cells were then further enhanced by cytokine activation (using IL-2 or GM-CSF) when these were either added directly into the culture media or genetically introduced or activated in these cultivated cells. More recently melanoma was the first tumor to be extensively treated by monoclonals directed at either CTLA-4 or PD-1/PD-L1 as agents for immune checkpoint blockade [21].
Prostate cancer has some similarities to melanoma. Each can remain dormant for long periods of time, are frequently treated by irradiation and express tumor associated antigens (gp100 by melanoma and prostate specific antigen [PSA], prostate specific membrane antigen [PSMA], prostatic acid phosphatase [PAP] and prostate cancer antigen-3 [PCA-3] by the prostate). Irradiated tumors shed antigens and provide recognition targets for activated T cells (unless inhibited by Treg suppressor cells). Immune checkpoint blockade works by several mechanisms which include targeting suppressive proteins (like CTLA-4) which interferes with the stimulatory interaction of T lymphocyte CD28 and B7 on antigen presenting cells. The result is continued anti-tumor immunologic responsiveness and prevention of tumor induced anergy and T cell tolerance. Such therapy could be employed following or in combination with gene therapy (including the use of antisense oligos). In addition to targeting the inhibitory signaling of T-cell CTLA-4, newer agents (also monoclonals) target the programmed death protein (PD-1) expressed by tumors, and its ligand (PD-L1) found on lymphocytes. When (or if) expressed, PD-1 acts as a tumor cloacking device, inhibiting specific cytotoxic lymphoid activity. If immune blockade therapy were to enter clinical trials for prostate cancer, these targets could be influenced by prior gene therapy and affect the ultimate outcome, therefore changes in expression must be taken into account and since immune checkpoint inhibitors only work in a small percentage of patients, prognostic indicators for their success much be identified, and ways to manipulate them found to increase the number of responsive patients.
Three FDA approved agents were initially approved to treat melanoma (Yervoy, Keytruda and Optiva). The first was directed against CTLA-4 (for which James Allison was awarded the 2018 Nobel Prize) and the latter two directed against the PD-1/ PD-L1 loop. Since their initial approval they have similarly been approved for a variety of solid and hematologic tumors as well. Against some cancers they are even being employed as the first and preferred agents to employ (i.e. melanoma).
Since oligo directed suppression of bcl-2 seems to alter so many metabolic pathways, most of which seem to indicate a transition to or selection of a more aggressive tumor type, we believe that immune regulation could be yet another pathway to evade therapy (particularly that directed towards bcl-2) through compensation. To test this theory in the current investigation we once again used RT- PCR to evaluate the immune regulatory markers for programmed death-1 (PD-1) and its ligand (PD-L1), in addition to a prognostic indicator (CDK-12) which is reported to identify prostate cancers susceptible (or not) to anti PD-1 immunotherapy [22].
Compensatory effects identified with these proteins are important since the PD-1/PD-L1 pathway is now recognized as a target for monoclonal antibody directed immunotherapy used to treat various solid tumors, particularly melanoma and lung tumors. However, immunotherapy is only effective for a relatively small percentage of patients, and prognostic indicators are needed to identify those patients most susceptible to it. One such prognostic indicator is CDK-12 which for prostate cancer can identify a subpopulation of patients susceptible to such checkpoint inhibitors [22]. In this study we evaluated both the expression of PD-1, PD-L1 and CDK- 12 expression following antisense inhibition using oligos directed towards bcl-2.
We employed RT-PCR in these experiments to determine alterations in gene expression. Although more sophisticated techniques are available, we find this method both sensitive enough to identify those genes involved with compensation and able to identify non-targeted genes (like KI-67, and the cyclins) [11] which are particularly affected and could provide combination targets for bcl-2 suppressive therapy. If compensation for bcl-2 suppression results in an increasingly aggressive, androgen sensitive and more rapidly proliferating tumor, increased expression of the proliferation marker KI-67 (or possibly the mitosis regulating cyclinD1) would most likely be the result of this process and could identify another target further intervention. Such proteins could even provide the second target on bispecific oligos; a role currently filled by a binding site for EGFR in these studies.
Methods
Oligonucleotides
Oligos (mono- or bispecific) were purchased from Eurofins MWG Operon (Huntsville, AL). Each was phosphorothioated on three terminal bases at 5’ and 3’ positions. Stock solutions were made to a final concentration of 625 μM in sterile Dulbecco PBS.
Base Sequences
Each oligo contained at least one CAT sequence and targeted the area adjacent to the mRNA AUG initiation codon for the respective targeted protein (EGFR or bcl-2).
MR4 (monospecific targeting bcl-2) T-C-T-C-C-C-A-G-C-G-T-G-C-G-C-C-A-T
MR24 (bispecific targeting EGFR/bcl-2) G-A-G-G-G-T-C-G-C-A-
T-C-G-C-T-G-C-T-C-T-C-T-C-C-C-A-G-C-G-T-G-C-G-C-C-A-T
MR42 (bispecific targeting bcl-2/EGFR) T-C-T-C-C-C-A-G-C- G-T-G-C-G-C-C-A-T-G-A-G-G-G-T-C-G-C-A-T-C-G-C-T-G-C- T-C
Cell Culture
LNCaP cells were grown in RPMI 1640 supplemented with 10% bovine serum, 1% L-glutamine and 1% penicillin/streptomycin in a 5% CO2 incubator. Log phase cells were harvested using EDTA/ trypsin and equally distributed into 75 cm2 flasks (Corning, NY). At intervals media were either supplemented or replaced with fresh.
Oligo Treatment Prior to PCR
Four days prior to oligo addition, when cell density approached 75% confluence, 10 ml of fresh media was added. Cells were incubated for an additional 3 days before 5 ml of media was replaced with fresh the day before oligos were added. 100 μl of stock oligos were added to bring the final concentration to 6.25 μM. Incubation proceeded for an additional 24 hours in the presence or absence of monospecific MR4, or the MR24 and MR42 bispecifics in a nanoparticle suspension with lipofectin.
RNA Extraction
Following treatment, media was removed, a single ml of cold (4oC) RNAzol B was added to each 75 cm2 culture flask and the monolayer lysed by repeated passage through a pipette. All procedures were performed at 4oC. The lysate was removed, placed in a centrifuge tube to which 0.2 ml of chloroform was added, and shaken. The mixture stayed on ice for 5 min, was spun at 12,000 g for 15 min, and the upper aqueous volume removed and placed in a fresh tube. An equal volume of isopropanol was added, the tube shaken, and allowed to stay at 4oC for 15 min before similar centrifugation to pellet the RNA. The supernatant was removed, the pellet washed in a single ml of 75% ethanol, then spun for 8 min at 7500 g. The ethanol was pipetted off and the formed pellet air dried at -20oC.
RNA Quantitation
RNA was resuspended in 250 μl of DEPC treated H2O, and quantitated using a Qubit fluorimeter and Quant-iT RNA assay kit (Invitrogen). DEPC is an inhibitor of RNase activity.
RT-PCR
Extracted RNA was diluted in DEPC treated water to 40 μg/μl. 1-4 μl of this RNA was added to1 μl of both sense and antisense primers (forward and reverse sequences) for bcl-2, actin, PD-1, PD-L1 and CKD-12.
From a kit purchased from Invitrogen the following reactants were added for RT-PCR: 25 μl of 2X reaction mixture, 2 μl SuperScript III RT / platinum Taq mix, tracking dye, and 3 μl MgSO4 (of a 5mM stock concentration). DEPC treated water was added to yield a final volume of 50 μl. RT-PCR was performed for 2 X 25 cycles using the F54 program in a Sprint PCR Thermocycler. As a control for RT-PCR product production, human actin expression was tested in RNA extracted from HeLa cells which was provided in a kit purchased from Invitrogen (in the reaction mixture, no MgSO4 was included, the difference compensated for by 3 μl of DEPC treated water).
Primers
Primer sequences were obtained from the National Center Biotechnology Information (NCBI) website: http://www.ncbi.nlm.nih.gov/nuccore/NM_031966
They were designed to amplify 100-300 bp fragments and anneal between 58-60oC.
Bcl-2
Forward primer sequence: 5’ GAG ACA GCC AGG AGA AAT CA 3’
Reverse primer sequence: 5’ CCT GTG GAT GAC TGA GTA CC 3’
PCR product produced was 127 base pairs in length.
Actin
Forward primer sequence: 5’ CAA ACA TGA TCT GGG TCA
TCT TCT C 3’
Reverse primer sequence: 5’ GCT CGT CGT CGA CAA CGG CTC
PCR product produced was 353 base pairs in length
PD-1
Forward primer sequence: 5’ GAC TAT GGG GAG CTG GAT TT 3’
Reverse primer sequence: 5’ AGA GCA GTG TCC ATC CTC AG 3’
PCR product produced was 192 base pairs in length.
PD-L1
Forward primer sequence: 5’ TGA TAC ACA TTT GGA GGA GAC G 3’
Reverse primer sequence: 5’ CCC TCA GGC ATT TGA AAG TAT C 3’
PCR product produced was 261 base pairs in length.
CDK-12
Forward primer sequence: 5’ GTC CAC TCC CCA GTA GGA AA 3’
Reverse primer sequence: 5’ ACA GGT GAA CCC TTG GAC TC 3’
PCR product produced was 241 base pairs in length
Detection and Quantitation of Product
Agarose Gel Electrophoresis
1.5% agarose gels were prepared in a 50 ml volume of TBE buffer (1X solution: 0.089 M Tris borate and 0.002M EDTA, pH 8.3), containing 3 μl of ethidium bromide in a Fisher Biotest electrophoresis system. Samples were run for 2 hours at a constant voltage of 70 using a BioRad 1000/500 power supply source. To locate the amplified PCR product, 3 μl of a molecular marker (Invitrogen) which contained a sequence of bases in 100 base pair increments (Invitrogen) as well as 2 μl of a sucrose-based bromophenol blue tracking dye were run in each gel.
Quantitation
Gels were visualized under UV light and photographed using a Canon 800 digital camera. Photos were converted to black and white format and bands quantitated using Medical Image Processing and Visualization (Mipav) software provided by the National Institute of Health. Means and standard deviations were compared using Student t-tests to determine significance.
Results
Bcl-2 Expression
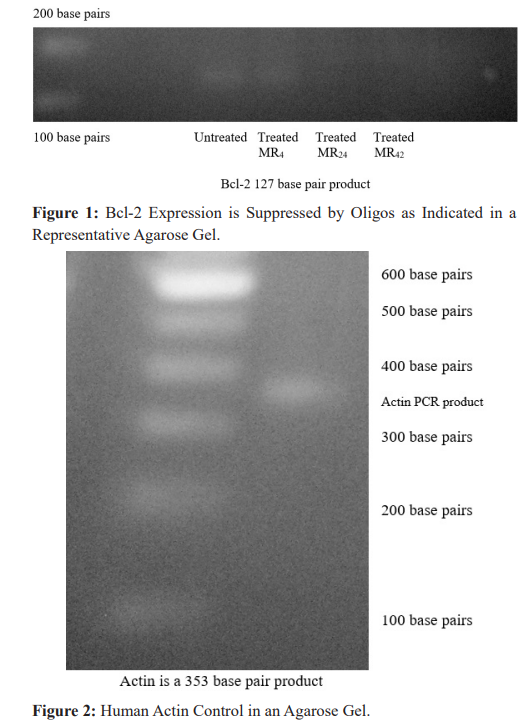
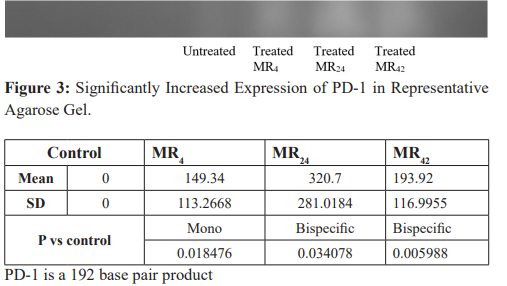
LNCaP cells incubated for 24 hours in the presence of 6.25 μM of oligos suppressed Bcl-2 expression, and support the finding of comparable biologic activity in both mono- and bispecific oligos measured in the in vitro cell growth inhibition experiments [16]. When photographs of the identified product bands were scanned on agarose gels and quantitated using Mipav software, in a series of runs, the greatest expression of bcl-2 was always found in untreated LNCaP cells. Those treated with oligos, whether mono-or bispecific, produced bands which indicated obvious (to the naked eye) suppression. For each oligo evaluated, the greatest amount of suppression measured approached 100% for the mono- specific MR4; and for the bispecifics MR24 and MR42, 86% and 100%, respectively. Suppression was found in both repeat PCR runs with bcl-2 primers, as well as in repetitive agarose gel quantification (Figure 1). As a control (data not shown) for RT- PCR product production, human actin expression was tested in RNA extracted from HeLa cells [11] (Figure 2).
PD-1 Expression
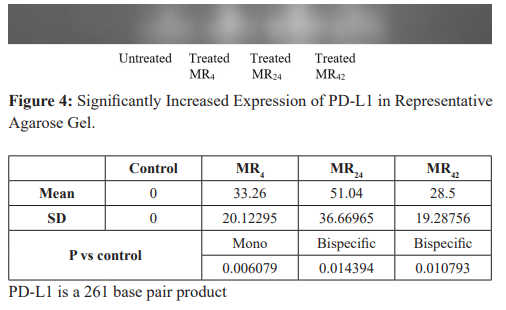
Comparable amounts of extracted RNA from LNCaP cells treated with either mono- or bispecific oligos directed against BCL-2 (and EGFR in the bispecifics) was then evaluated by RT-PCR using primers directed against PD-1. When background intensity was subtracted, the relative intensity of the bands corresponding to PD- L1 representing cells treated with MR4, MR24 and MR42 compared to controls were increased 149.3% ± 113.3 (P = 0.018476), 320.7% ±281.0 (P = 0.034078), and 193.9% ± 117.0. (P = 0.005988) (mean± SD). These results indicate that the expression of the immune blockade marker PD-1 is significantly enhanced suggesting once again another compensatory response to bcl-2 suppression may occur. A representative band is presented in Figure 3.
PD-L1 Expression
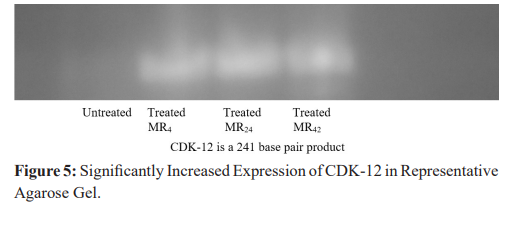
Comparable amounts of extracted RNA from LNCaP cells treated with either mono- or bispecific oligos directed against bcl-2 (and EGFR in the bispecifics) was then evaluated by RT-PCR using primers directed against PD-L1.
When background intensity was subtracted, the relative intensity of the bands corresponding to PD-L1 representing cells treated with MR4, MR24 and MR42 compared to controls were increased 33.3% ± 20.1 (P = 0.006079), 51.0% ± 36.7 (P = 0.014394), and 28.5% ± 19.3 (P = 0.010793) (mean ± SD). These results indicate that the expression of the immune blockade marker PD-L1 is significantly enhanced (to lesser extent), suggesting once again another compensatory response to bcl-2 suppression may occur. A representative band is presented in Figure 4.
CDK-12 Expression
As seen in a representative band in Figure 5, CDK-12 is not well expressed (if at all) in untreated LNCaP cells, which would suggest that this tumor line would be susceptible to immunotherapy [22]. However, in light of the increased expression of both PD-1 and PD- L1, it is increasingly clear that immunotherapy is very complex and that antisense directed against a completely non-related gene (like bcl-2) can produce significant and unanticipated effects elsewhere. One would have thought that the increased PD-1 expression that results from oligos directed against bcl-2 would have made the tumor cell a better target for immunotherapy, which would be our first finding where compensation would help a potential patient, while potentiating an anti-tumor immune response. However, it appears that the massive increase in CDK-12 expression in these same cells would at least compromise or completely eliminate this benefit.
Discussion
Gene therapy is often promoted as a highly specific and deliverable treatment to control aberrant gene expression by tumor cells (particularly when growth factors, their receptors, apoptosis inhibitors or oncogenes are excessively transcribed). However, it’s now apparent that it’s not as specific as previously believed.
Antisense oligos consist of nucleotide bases synthesized complimentary in sequence to mRNA. When hybridized to mRNA, they produce a translational arrest of the targeted gene’s mRNA expression. This method is an effective, relatively non- toxic and inexpensive form of therapy and various types of antisense RNA have been constructed for this purpose. These include the phosphorothioated oligos used in these evaluations and other formulation including 2’-MOE-RNA, morpholinos, siRNA, miRNA etc. Modifications to the oligo backbone and base structure are used to prevent nuclease degradation, increase systemic half- life and to enhance distribution and delivery, particularly across the blood: brain barrier. Some of these derivatives have been evaluated in clinical trials, but all oligos employed were directed against single gene transcriptional (mRNA) products. In contrast, the oligos discussed in this paper included both mono- and bispecific forms, each having a base sequence complementary to and directed against mRNA encoding the apoptosis inhibitor bcl-2, (bispecifics included an additional site directed against EGFR). We evaluate bispecific oligos because it would be naïve to believe targeting a single mRNA would be sufficient to produce a clinical response in most tumors, and activity at one site does not affect binding at a second [16]. Furthermore we have shown that both mono- and bispecific oligos have comparable activity when suppressing bcl-2 [16]. Therefore administration of a single oligo having two mRNA targets could have an additional suppressive benefit, particularly if EGFR is excessively produced (when using these bispecifics).
While it’s understandable that unrelated genes which share sequence homology would also be susceptible to antisense oligos, when directed towards that common sequence, what is not expected are the effects on non-targeted genes having unrelated sequences; many of which control additional growth regulating pathways, and as we now believe regulate the immune response, as well.
In addition to unanticipated effects upon unrelated genes either having or not containing related sequences; we have also shown that certain complementary stretches of base sequences can occur within the oligo itself which can also produce unanticipated effects affecting the immune system. Complementary intra strand binding has been shown to increase the expression of interferon which may have a role in the expression of cell surface antigens and differentiation proteins, like PSA or PSMA. In an early evaluation of bispecifics we reported the enhanced expression of PSMA [6] when oligos were directed against bcl-2. The unique capacity to produce such changes by these bispecfics (and not a similarly directed monospecific) is attributable to an unusual double strand conformation present in bispecifics and interferon induction (an enhancer of surface antigen expression, like PMSA) [6]. Such expression could enable better recognition and targeting by cytotoxic T cells toward cell surface PSMA [6]; to a greater extent than secretory PSA or PAP.
Tumors are a mass of genetically unstable heterogeneous cells capable of both rapid mutation and selection. As noted above, compensation for suppression of bcl-2 also leads to greater chromosomal instability and gene fusion involving TMPRS22 [10] and fusion transcription protein FLI-1 [11]. All this leads to greater proliferation and mitosis as indicated by KI-67 and cyclin D1 [11]. Therefore, just as bacterial and viral agents develop resistance to chemotherapeutics, tumors cells have a similar capability.
Initial evaluation of protein expression associated with compensation regulating the traditional mode of apoptosis (mitochondrial mediated) focused on the bcl-2, bax, bad, clusterin etc. However, more recent work evaluated proteins associated with tumor cell destruction, via apoptosis, mediated by a secondary route for activation, involving direct signal transduction. This is a process of initiating apoptosis through the binding of activating proteins (ligands, like PD-L1) on immune cells to cell surface receptors (like tumor cell PD-1). When ligands bind to these receptors, they activate a destructive cascade of protein interactions which lead to cell death. These receptors are structurally similar to the tumor necrosis factor receptor (CD95) and also regulate the immune system’s cytotoxic T cell response.
We conclude that the increase in CDK-12 expression following treatment would suggest a resistance to immunotherapy, not present in the untreated LNCaP cells; and follow the pattern that compensation for antisense oligos directed towards bcl-2 make tumors more aggressive, androgen sensitive and proliferative. However, one would have thought that the increased PD-1 expression that results from oligos directed against bcl-2 would have made the tumor cell a better target for immunotherapy. That PD-1 its ligand PD-L1 and CDK-12, were all significantly enhanced following bcl-2 suppression suggest that immunoregulation, is an additional pathway for compensatory based resistance. It is also obvious that, there is much to learn regarding the non-specific effects of gene therapy in general and antisense oligos oligos in particular. As demonstrated here, findings can at times be counter- intuitive unless the massive increase in CDK-12 expression in these same cells would overwhelm the apparently advantage of increased PD-1 expression.
This year (2019) the American Cancer Society (ACS) estimated that in spite of early detection, screening for prostate specific antigen (PSA) and effective treatments for localized disease, in the United States there are 31,620 expected deaths from prostate cancer with 174,650 newly diagnosed cases [23]. New types of treatment, including gene therapy and translational inhibition must be developed and employed (probably in combination with traditional androgen ablation).
Acknowledgments
The Cellular Biology laboratory at the Hektoen Institute is supported, in part, by the Blum Kovler Foundation, the Cancer Federation, Safeway/Dominicks Campaign for Breast Cancer Awareness, Lawn Manor Beth Jacob Hebrew Congregation, the Max Goldenberg Foundation, the Pritzker Traubert Family Foundation, the Janet Rubenstein Memorial Foundation, the Sternfeld Family Foundation, and the Herbert C. Wenske Foundation.
References
- Rubenstein M, Dunea G, Guinan P. Growth factor deprivation therapy utilizing antisense Drug News and Perspectives. 1994; 7: 517-524.
- Rubenstein M, Mirochnik Y, Chow P, et Antisense oligonucleotide intralesional therapy of human PC-3 prostate tumors carried in athymic nude mice. J Surg Oncol. 1996; 62: 194-200.
- Rubenstein M, Mirochnik Y, Chou P, et Growth factor deprivation therapy of hormone insensitive prostate and breast cancers utilizing antisense oligonucleotides. Meth Find Clin Pharmacol. 1998; 20: 825-831.
- Yamanaka K, Miyake H, Zangemeister-wittke U, et Novel bispecific antisense oligonucleotides inhibiting both bcl-2 and Bcl-xL expression induce apoptosis and enhance chemosensitivity in human androgen- independent prostate cancer cells. Proceedings AACR 45.2004.
- Yip KW, Mocanu JD, Au PY, et Combination bcl-2 antisense and radiation therapy for nasopharyngeal cancer. Clin Cancer Res. 2005; 11: 8131-8144.
- Rubenstein M, Hollowell CMP, Guinan Bispecific oligonucleotides may induce interferon in LNCaP cells enhancing surface antigen expression: Effect of intra strand base pair complementarity. In Vivo. 2011; 25: 61-67.
- Rubenstein Suppression of bcl-2 by antisense oligonucleotides is compensated through increased activity of the androgen receptor and co-activators but not 5-alpha reductase. Cancer Research and Oncology: Open Access. 2016; 2.
- Rubenstein M, Hollowell CMP, Guinan Following inhibition of BCL-2 by antisense oligonucleotides compensatory suppression of apoptosis involves the direct signal transduction pathway of LNCaP cell. Online Journal of Apoptosis. 2015; 4: 1-10.
- Rubenstein M, Hollowell CMP, Guinan Oligonucleotide suppression of bcl-2 in LNCaP cells is compensated by increased androgen sensitivity, p53 and oncogene activity, and suppressed caspase-3. Med. Oncol. 2013; 30: 599.
- Rubenstein M. Expression of TMPRSS22, androgen receptor and its co-activators are increased following suppression of bcl-2 by antisense oligonucleotides: But the TMPRSS22 fusion partner ERG is not detectable in the compensatory response. Cancer Research and Oncology: Open 2016; 2: 022.
- Rubenstein Mechanisms by Which Non-targeted Genes Compensate for Specific Gene Therapy Directed Towards Bcl-2 in a Prostate Cancer Model. eBook: Recent Advances in Prostate Cancer. 2017; 2.
- Rubenstein M, Mirochnik Y, Chou P, et Growth factor deprivation therapy of hormone insensitive prostate and breast cancers utilizing antisense oligonucleotides. Meth. Find Clin Pharmacol. 1998; 20: 825-831.
- Oncogenex website: Oncogenex.ca
- Rubenstein M, Mirochnik Y, Ray V, et Lack of toxicity associated with the systematic administration of antisense oligonucleotides for treatment of rats bearing LNCaP prostate tumors. Med Oncol. 1997; 14: 131-136.
- Rubenstein M, Tsui P, Guinan Bispecific antisense oligonucleotides with multiple bindings sites for the treatment of prostate tumors and their applicability to combination therapy. Meth. Find Clin Pharmacol. 2006; 28: 515-518.
- Rubenstein M, Guinan P. Bispecific antisense oligonucleotides have activity comparable to monospecifics in inhibiting expression of Bcl-2 in LNCaP In Vivo. 2010; 24: 489-493.
- Rubenstein M, Hollowell CMP, Guinan Inhibition of bcl-2 by antisense oligonucleotides is followed by a compensatory suppression of caspase-3 in LNCaP cells. Eur J Clin Med Oncol. 2011; 3: 1-6.
- Rubenstein Suppression of bcl-2 by antisense oligonucleotides is compensated through increased activity of the androgen receptor, variants (ARv7 and ARv9) and several co-activators. Oncol Res Rev. 2018; 1: 1-7.
- Rubenstein M, Hollowell CMP, Guinan In LNCaP cells enhanced expression of both androgen receptor and co-stimulatory protein p300 compensate for antisense oligonucleotide suppression of bcl-2 Ther. Adv. Urology. 2011; 3: 243-250.
- Rubenstein M, Hollowell CMP, Guinan Additional compensatory mechanisms -altering antisense oligonucleotide suppression of Bcl-2: Effects upon AKT-1 and STAT.-3. In Vivo. 2014; 28: 867-870.
- http://www.washingtonpost.com/business/studies-merck-drug-keytruda-effective-against-3-cancers/2015/04/19/01d94cfc-e6b4-11e4-8581-633c536add4b_story.html
- Furlow CDK-12 loss a biomarker for prostate cancer response to immunotherapy. Cancer and Genetics News Prostate Cancer. 2018.
- American Cancer Cancer Facts & Figures. Atlanta: American Cancer Society. 2019.