Effects of Transcutaneous Electrical Nerve Stimulation on Pain Control in Patients with Knee Osteoarthritis a Systematic Review
Author'(s): Lee H*, Clark A and Draper DO
Brigham Young University, Provo, UT 84602
*Correspondence:
Lee H, Brigham Young University, Provo, UT 84602.
Received: 09 November 2020; Accepted: 29 November 2020
Citation: Lee H, Clark A, Draper DO. Effects of Transcutaneous Electrical Nerve Stimulation on Pain Control in Patients with Knee Osteoarthritis a Systematic Review. Anesth Pain Res. 2020; 4(3): 1-4.
Keywords
Introduction
Knee osteoarthritis (OA), which causes knee joint pain, stiffness, and functional disability [1], is common among elderly individuals [2]. A literature search suggested that 27.8% of individuals aged over 45 years old had a prevalence of radiographic knee OA grade of at least 2 in at least 1 knee and 43.3% had symptomatic knee pain, aching, or stiffness in at least 1 knee [3]. There is no perfect treatment or measures for knee OA patients up to date. Therefore, pain therapy is considered as a main treatment for those with knee OA.
Transcutaneous electrical nerve stimulation (TENS) is a commonly used conservative treatment method that is effective in reducing knee pain in patients with knee OA [4-6]. However, it is still controversial in effectiveness of TENS based on randomized controlled trials (RCTs) and systematic reviews compared with healthy control groups [7-9]. Therefore, it is effective in decreasing knee pain. In addition, the main outcome of the literature on TENS is level of knee pain, which was measured using instruments such as the visual analog scale (VAS) or Western Ontario and McMaster Universities Arthritis Index scale (WOMAC). Decrease in pain can lead improved normal physical function; however, limited studies have reported the effect of decrease in pain on physical function through factors such as muscle strength, speed, endurance, and balance. Further, it is been limited to confirm if TENS intervention is effective in reducing pain and developing physical tests [10,11].
In the previous studies, they have suggested that discrepancy between physical symptom and radiographic evaluation. The K/L grade is a common radiographic evaluation system for knee OA; it involves classification of knee OA according to the severity of bone deformity [12]. However, there was no statistically significant relationship between K/L grade and knee pain [13], leg extensor and flexor muscle strengths, and WOMAC [14,15]. In addition, people with K/L score 0 may have cartilage damage or bone marrow lesions, as demonstrated using magnetic resonance imaging [16]. There is possibility that even people with K/L grade 0 or 1 (preradiographic OA) have inadequate function and/or knee pain. Additionally, those with preradiographic OA, particularly with K/L grade 1, have been expected to develop to at least grade [2,17,18]. Moreover, another previous study reported that people with early-stage knee OA have higher possibility of having better response to treatment than those with late-stage knee OA [19].
Therefore, the purpose of this systematic review with meta- analysis was to determine whether TENS can alleviate joint pain in patients with knee OA. On the basis of the existing literature, we hypothesize that TENS treatment is effective in reducing joint pain for knee OA patients.
Methods
We searched PubMed, CINAHL, SPORT Discus, and Scopus databases from their earliest available date to March 2016 using the combination of key words, including 1) joint pain OR knee osteoarthritis OR TENS OR pain control OR 2) ACLR OR ACL injury; and 3) items 1 AND 2.
Inclusion and exclusion criteria
After the initial electronic search, duplicated articles were eliminated by comparing the results from each database. On the basis of title and abstracts, articles returned that were not relevant and English language, full text, or original articles were rejected [1-19].
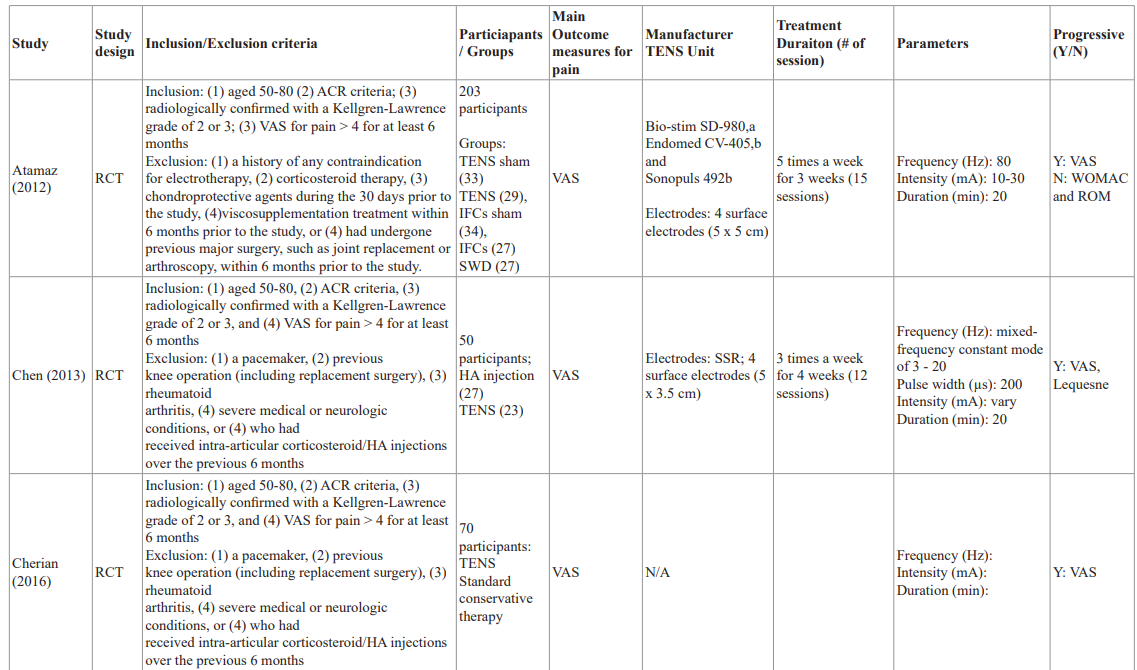
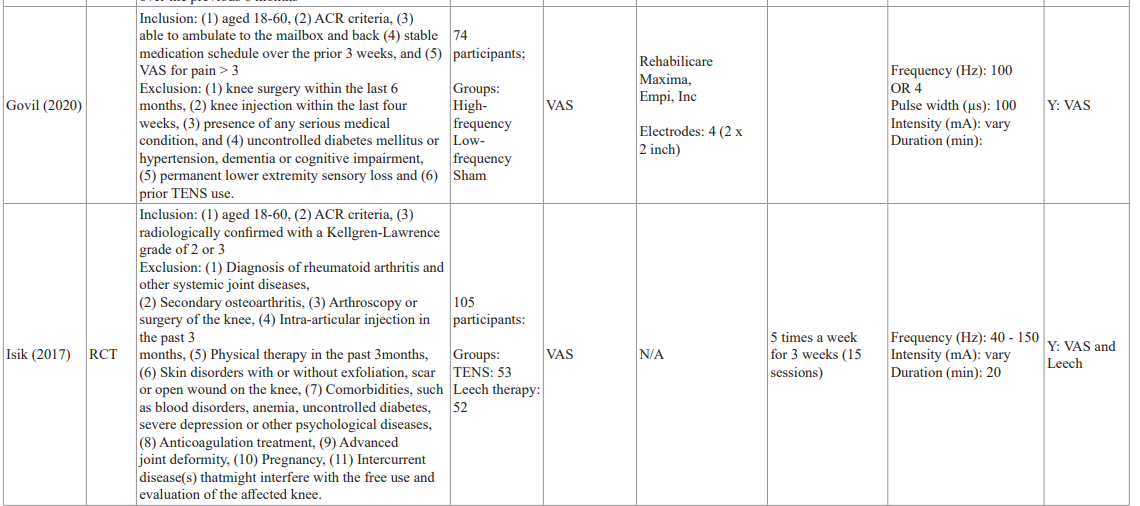
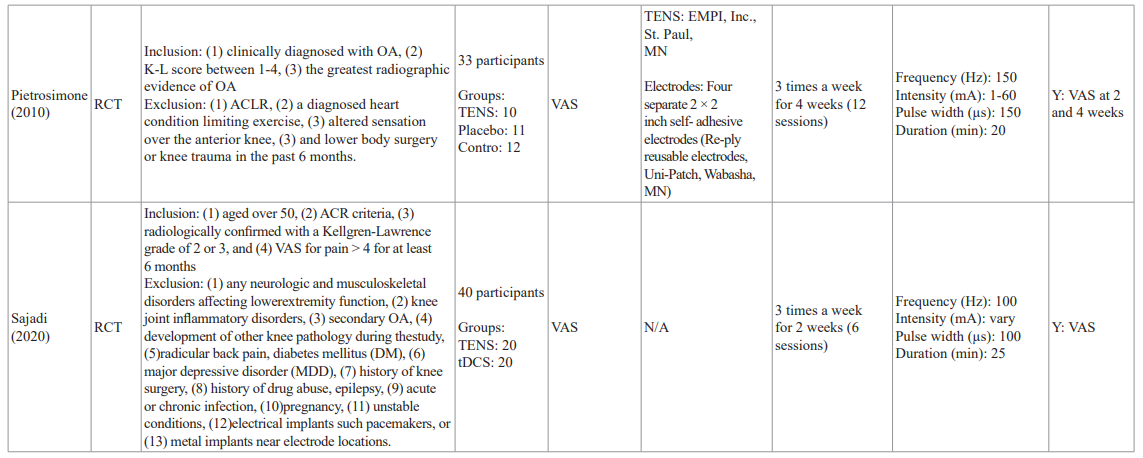
The authors independently made the initial selection based on the titles and abstracts of the papers. Any disagreement between the 2 authors was resolved by discussion. If there was still debate, a third reviewer (S.-Q.F.) was consulted and made a decision regarding its inclusion. Information including the authors, study design, mean age, sex, study population, stimulation frequency (of TENS), outcome measures, and follow-up periods were extracted from each included study.
Discussion
The systematic review is the first to pool data from individual studies on the effects of TENS on pain control in patients with knee OA. The results provide evidence that TENS treatments are effective in reducing self-reported pain level. More specifically, the TENS treatments, 12-15 sessions over 4-6 weeks, reduce VAS in pain right after the treatments and it lasts about 2 weeks. However, it did not show how long the effect lasted after 2 weeks. Different physical therapy approaches have been used to develop the clinical course of knee OA, but the evidence of effectiveness has not been sufficient based on randomized controlled studies and analyzed by a systematic review.
TENS is effective for nociceptive pain mechanisms based on the gait control theory of pain [20] and activation of endogenous opioids, and it may improve exercise tolerance in individuals who experience movement-evoked pain. Shimoura et al. [21] reported that TENS intervention was considered to reduce knee movement- evoked pain and increase walking distance without pain. Thus, participants in the TENS group may be able to walk longer distances in the post-assessment period. According to Isik’s [22] study, they compared a three-session leech therapy applied on ambulatory patients with a routinely applied full term TENS therapy which involved 15 sessions of TENS therapy application on hospitalized patients in 3 weeks. In the evaluation of the main outcome scores on day 21st, pain score in VAS significantly decreased in both groups which were consistent with previous studies. In addition, Pietrosimone et al. [23] stated that although significant differences were not found between groups, moderate TENS effect sizes were found 4-weeks following the initiation of the intervention. In the most recent article in this systematic review, significant analgesic effect and functional improvement were observed in patients who received TENS.
Based on the RCTs in our systematic review, TENS decreases pain in patients with knee OA. Previous authors have concluded that the neural drive is immediately increased during the active administration of sensory TENS current, and that TENS immediately diminished the excitatory effect upon removal. Current theories suggest that TENS provides increased afferent stimuli interpreted by the CNS as excitatory resulting in the facilitation of inhibited motor neuron pools.
In conclusion, this systematic review indicated that: (1) patients who received TENS had significantly decreased pain compared with the control group; (2) there was no significant difference between the TENS and control groups in terms of the WOMAC index and all-cause discontinuation; (3) there was no significant difference between the TENS and control groups in the pain- limited ROM and/or total passive knee ROM; and (4) TENS might significantly improved the maximum knee ROM on day 10 and during follow-up compared with the control group.
References
1.Richmond J, Hunter D, Irrgang J, et al. Treatment of osteoarthritis of the knee (nonarthroplasty). J Am Acad Orthop Surg. 2009; 17: 591-600.
2.Woolf AD, Pfleger B. Burden of major musculoskeletal conditions. Bull World Health Organ. 2003; 81: 646-656.
3.Jordan JM, Helmick CG, Renner JB, et al. Prevalence of knee symptoms and radiographic and symptomatic knee osteoarthritis in African Americans and Caucasians: the Johnston County Osteoarthritis Project. J Rheumatol. 2007; 34: 172-180.
4.Chen WL, Hsu WC, Lin YJ, et al. Comparison of intra-articular hyaluronic acid injections with transcutaneous electric nerve stimulation for the management of knee osteoarthritis: a randomized controlled trial. Arch Phys Med Rehabil. 2013; 94: 1482-1489.
5.Cherian JJ, Kapadia BH, McElroy MJ, et al. Knee osteoarthritis: does transcutaneous electrical nerve stimulation work? Orthopedics. 2016; 39: 180-186.
6.Chen L-X, Zhou Z-R, Li Y-L, et al. Transcutaneous electrical nerve stimulation in patients with knee osteoarthritis. Clin J Pain. 2016; 32: 146-154.
7.Atamaz FC, Durmaz B, Baydar M, et al. Comparison of the efficacy of transcutaneous electrical nerve stimulation, interferential currents, and shortwave diathermy in knee osteoarthritis: a double-blind, randomized, controlled, multicenter study. Arch Phys Med Rehabil. 2012; 93: 748- 756.
8.Palmer S, Domaille M, Cramp F, et al. Transcutaneous electrical nerve stimulation as an adjunct to education and exercise for kneeosteoarthritis: a randomized controlled trial. Arthritis Care Res (Hoboken). 2014; 66: 387-394.
9.Zeng C, Li H, Yang T, et al. Electrical stimulation for pain relief in knee osteoarthritis: systematic review and network meta-analysis. Osteoarthritis Cartilage. 2015; 23: 189-202.
10.Nakamura K. A “super-aged” society and the “locomotive syndrome.” J Orthop Sci. 2008; 13: 1-2.
11.Japanese Orthopaedic Association. Locomotive syndrome. In: Locomotive Challenge! Council, editors. Locomotive syndrome pamphlet. 2013.
12.Kellgren JH, Lawrence JS. Radiological assessment of osteo-arthrosis. Ann Rheum Dis. 1957; 16: 494-502.
13.Felson DT, Zhang Y, Hannan MT, et al. The incidence and natural history of knee ostoathritis in the elderly. The Framingham Osteoarthritis Study. Arch Rheum. 1995; 38: 1500-1505.
14.Tuna S, Balci N. The relationship between radiological severity and functional status in patients with knee osteoarthritis. Clin Rheumatol. 2014; 33: 667-670.
15.Ruhdorfer A, Wirth W, Hitzl W, et al. Association of thigh muscle strength with knee symptoms and radiographic disease stage of osteoarthritis: data from the osteoarthritis initiative. Arthritis Care Res (Hoboken). 2014; 66: 1344-1353.
16.Guermazi A, Niu J, Hayashi D, et al. Prevalence of abnormalities in knees detected by MRI in adults without knee osteoarthritis: population based observational study (Framingham Osteoarthritis Study). BMJ. 2012; 345: 5339.
17.Hart DJ, Spector TD. Kellgren & Lawrence grade 1 osteophytes in the knee–doubtful or definite? Osteoarthritis Cartilage. 2003; 11: 149-150.
18.Cibere J, Sayre EC, Guermazi A, et al. Natural history of cartilage damage and osteoarthritis progression on magnetic resonance imaging in a population-based cohort with knee pain. Osteoarthritis Cartilage. 2011; 19: 683-688.
19.Bruyere O, Cooper C, Arden N, et al. Can we identify patients with high risk of osteoarthritis progression who will respond to treatment? A focus on epidemiology and phenotype of osteoarthritis. Drugs Aging. 2015; 32: 179-187.
20.Melzack R, Wall PD. Pain mechanisms: a new theory. Science. 1965; 150: 971-979.
21.Shimoura K, Iijima H, Suzuki Y, et al. Immediate effects of transcutaneous electrical nerve stimulation on pain and physical performance in individuals with preradiographic knee osteoarthritis: A randomized controlled trial. Archives of Physical Medicine and Rehabilitation. 2019; 100: 300-306.
22.Isik M, Ugur M, Yakisan RS, et al. Comparison of the effectiveness of medicinal leech and TENS therapy in the treatment of primary osteoarthritis of the knee. Zeitschrift für Rheumatologie. 2017; 76: 798-805.
23.Pietrosimone BG, Saliba SA, Hart JM, et al. Contralateral effects of disinhibitory TENS on quadriceps function in people with knee osteoarthritis following unilateral treatment. North American journal of sports physical therapy. 2010; 5: 111-121.