Emergency Sternotomy for Ruptured Left Ventricular Aneurysm A Case Report From the André Festoc Center at the “Le Luxembourg” Mother and Child Hospital in Bamako, Mali
Author'(s): Diarra BI1*, Doumbia M1, Tangara S1, Coulibaly BD1, Keita A3>, Daffe S2, Sidibé AS1, Doucouré O1,Coulibaly BM1, Traoré K1, Touré F1, Traoré S1, Diallo B1, Koita SS1-3, Togola B3, Togo S3,4, Ouattara MA3,4,,Yena S3,4, Fernandez G5, Nadjeeboulah B5, Flecher E5, Langanay T5, Amerin C5, Boutin L5 and Deloche A5
1Thoracic and Cardio-Vascular Surgery Department (Andre Festoc Center, Bamako, Mali).
2Cardiology Department of the "Luxembourg" Mother-Child Hospital in Bamako, Mali.
3Faculty of Medicine and Odontostomatology, University of Technical Sciences and Technologies of Bamako, Mali.
4Thoracic Surgery Department « Opital Du Mali ».
5Non-Governmental Organization Chain of Hope, France.
*Correspondence:
Dr. Baba Ibrahima DIARRA, cardio-vascular and thoracic surgeon, Phone: 00 223 93 33 63 96.
Received: 05 May 2024; Accepted: 08 Jun 2024; Published: 15 Jun 2024
Citation: Diarra BI, Doumbia M, Tangara S, et al. Emergency Sternotomy for Ruptured Left Ventricular Aneurysm A Case Report From the André Festoc Center at the “Le Luxembourg” Mother and Child Hospital in Bamako, Mali. Anesth Pain Res. 2024; 8(2): 1-4.
Abstract
Left ventricular aneurysm is rare. It can be spontaneous or acquired, appearing most often after a transmural myocardial infarction but can also follow cardiac operations, trauma, inflammation or infection [1]. We report the first case of a patient initially referred by the cardiology department of the CHU-ME for the surgical management of a large pericardial effusion whose immediate operative consequences were complicated by significant hemorrhage through the pericardial drain, prompting an emergency sternotomy, surgical exploration of which revealed a ruptured left ventricle aneurysm in a 14-year-old boy. In conclusion surgical repair of left ventricular aneurysm can be performed with acceptable results.
Keywords
Introduction
Vertical median sternotomy is the anterior approach to the thorax, providing access to the anterior mediastinum. A surgical emergency is any situation requiring immediate surgical intervention to rescue a person whose functional or vital prognosis is likely to be compromised. A left ventricular aneurysm is a localized, permanent dilatation of the left ventricular wall due to loss of parallelism. The etiologies are numerous: ischemia 55%, surgery 33%, trauma 7%, and infection 5%.
The aim of this work is to report the case of a patient initially referred for surgical management of a large pericardial effusion, whose immediate post-operative course was complicated by severe bleeding through the pericardial drain, prompting emergency sternotomy. Surgical exploration revealed a left ventricular aneurysm in contained rupture.
Observation
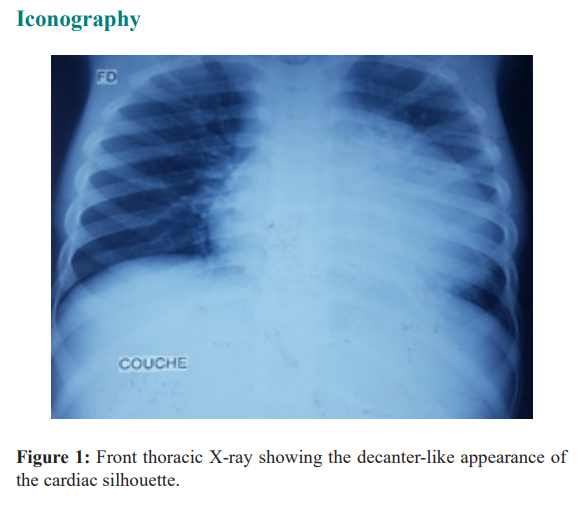
14-year-old patient with no medical or surgical history initially referred by the cardiology department for management of a pericardial effusion secondary to a sports accident trauma. He presented with an altered general condition (stage III of the World Health Organization classification), chest pain and NYHA dyspnea III, which had been evolving for three weeks. On auscultation, the heartbeat was muffled and rapid. Chest X-ray revealed an enlarged mediastinum (Figure 1).
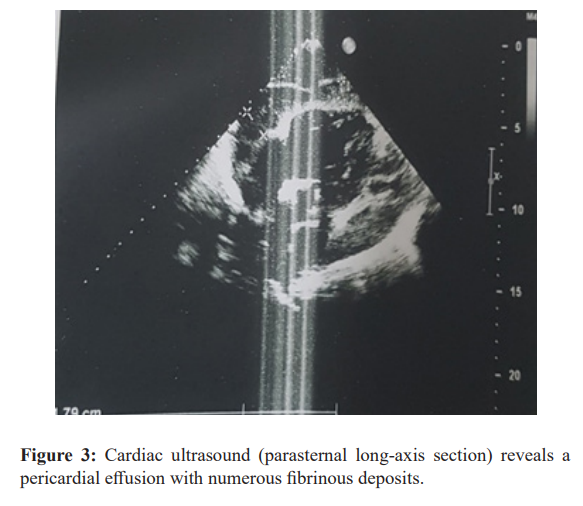
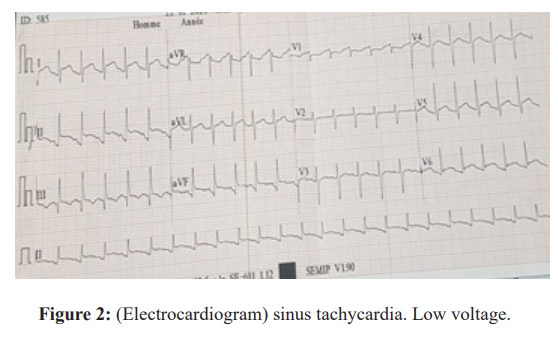
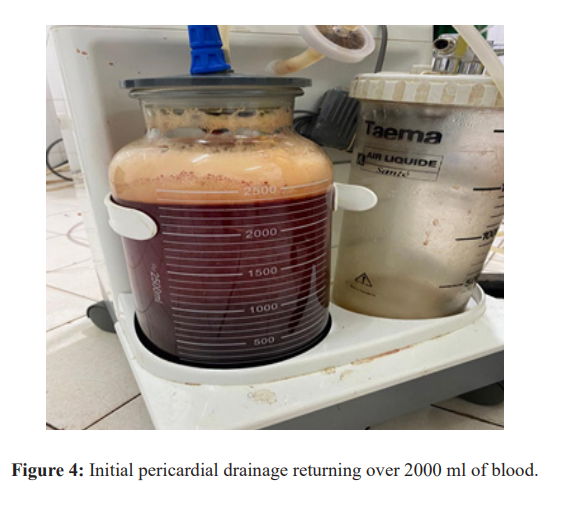
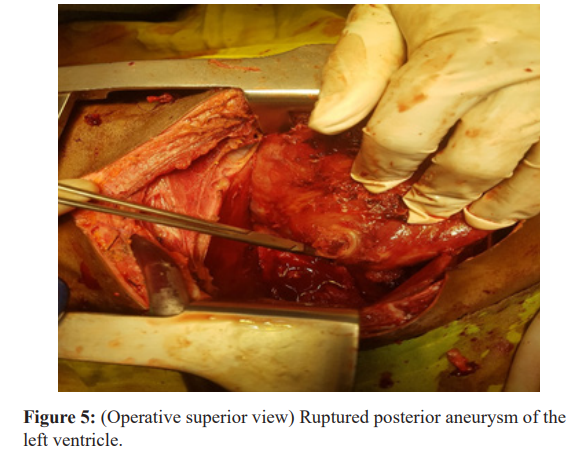
The electrocardiogram showed sinus tachycardia at 150 beats/min, and the trans-thoracic (Figure 2) Echocardiogram showed a large pericardial effusion with numerous fibrinous lesions (Figure 3). He was admitted to the emergency operating room for subxiphoid pericardial drainage using the Jaboulay technique under general anaesthesia with orotracheal intubation. The immediate post- operative course was marked by the occurrence of very significant hemorrhagic production through the drain, at a rate of 2000ml in 30 minutes (Figure 4). This prompted immediate clamping of the drain and emergency sternotomy. Surgical exploration revealed an abundant hemopericardium and a ruptured left ventricular aneurysm. The procedure consisted in performing a 4/0 prolene bursa reinforced with pledget stitches (Figure 5). In terms of resuscitation, he benefited from a transfusion of three bags of
Discussion
LV aneurysms are rare. They were first described in 1757 by John Hunter. Echocardiography-Doppler is the first-line examination and can establish the diagnosis with certainty [2]. Unlike true aneurysms, which have a resistant fibrosed wall and a wider neck, false aneurysms initially consist of loose tissue and a narrower neck [3,4]. Left ventricular aneurysms can be spontaneous or acquired, and in the latter case most often appear after transmural myocardial infarction, but can also arise following cardiac surgery, trauma, inflammation or infection [5]. Traumatic LV aneurysms account for 7% of all aneurysms [6]. Post-traumatic origin is most often due to open trauma, but cases of false aneurysm after closed trauma have been described [7], as in our case. The age of our patient was 14, which is comparable to the extreme age of children operated on for left ventricular aneurysms. The indication for surgery remains formal in the event of diagnosis of a false aneurysm, as the risk of rupture is high [8].
Once the diagnosis has been confirmed, surgical intervention should be proposed. Classically, this is based on patch repair under extracorporeal circulation via median sternotomy, although the beating-heart thoracotomy approach in cases of redux has been reported in the literature, making it possible to improve left ventricular hemodynamics by reducing its size, as well as preventing long-term remodeling [9]. The first surgery was performed in 1958 by Denton COOLEY under extracorporeal circulation.
There are many surgical techniques: linear sectioning by vertical ventricular incision into the aneurysm, endocavitary patch repair, Cooley's technique of septal plication with separate stitches [11], Dor's circular endoventricular plasty [12], Jatène's double-layer suture from one side of the aneurysm to the other [13].
Post-operative mortality in left ventricular pseudoaneurysms is accepted to be 13%-29% [10], but surgical intervention remains a priority for most teams because of the severity and spontaneously
Conclusion
Pericardial drainage can lead to emergency sternotomy. Emergency sternotomy is a specialized surgical procedure, and requires an adapted technical platform. Our case demonstrated the etiological complexity and management difficulties of left ventricular aneurysms. Surgical repair of left ventricular aneurysms can be performed with encouraging results.
References
- Miandrisoa Rev Anesth Réanim Med Urg Toxicol. 2018; 10: 11-13.
- Ndiaye MB, Ba FG, Bodian M, et al. Faux anévrisme du ventricule gauche du sujet jeune: à propos de trois cas. Ann Cardiol Angeiol. 2015; 64: 300-304.
- Mackenzie JW, Lemole GM. Pseudoaneurysm of the left ventricle. Tex Heart Inst J. 1994; 21: 296-301.
- Prêtre R, Linka A, Jenni R, et al. Surgical treatment of acquired left ventricular pseudoaneurysms. Ann Thor Surg. 2000; 70: 553-537.
- Chraibi S, Beghetti M, El Hattaoui M, et al. Faux anévrisme après ligature d’un canal artériel opéré avec succès. Ann Cardiol Angeiol. 2003; 52: 188-190.
- Frances C, Romero A, Grady Left ventricular pseudoaneurysm. J Am Coll Cardiol. 1998; 32: 557-561.
- Ben Omrane S, Zribi H, Rjeb MA, et al. Faux anévrisme du ventricule gauche après un traumatisme fermé du thorax (à propos d’un cas). Ann Cardiol Angeiol. 2008; 57: 231-233.
- Guihaire J, Verhoye JP, Flecher E, et al. Faux anévrismes du ventricule gauche après vidéothoracoscopie: à propos d’un cas. Chir Thorac Cardiovasc. 2009; 13: 120-123.
- Chukwumere E, John M, Richard M, et Surgical approach to myocardial rupture after acute myocardial infaction. Asian Cardiovasc Thorac Ann. 1998; 6: 108-114.
- Figueras J, Cortadellas J, Domingo E, et Survival following self limited left ventricular free wall rupture during myocardial infarction. Management differences between patients with or without pseudoaneurysm formation. Int J cardiol. 2001; 79: 103-111.
- Cooley DA, Collins HA, Morris GC. Anévrisme du ventriculaire après infarctus du myocarde
- Dor V, Saab M, Coste P, et anévrisme ventriculaire gauche:une nouvelle approche chirurgicale.
- Jatene Anévysmectomie ventricule gauche: résection our econstruction. Chirurgie cardiovasculaire J Thomac. 1985.