Epidemiological, Diagnostic, Therapeutic and Evolutionary Aspects of Late-Presenting St Segment Elevation Myocardial Infarction (STEMI): About 50 Cases Collected in Four Cardiology Departments in Dakar
Author'(s): Momar Dioum1*, Papa Guirane Ndiaye2, Louise Héléne Ndiaye1, Joseph Salavador Mingou3 , Saguinatou D. AW1 , Serigne Cheikh Tidiane Ndao4, Mohamed Gazaal2, Mouhamed C. Mboup4 and Maboury Diao4
1Fann University Hospital Cardiology Department, Dakar, Senegal.
2Hospital General Idrissa Pouye, Dakar, Senegal.
3Hospital Aristide Le Dantec, Dakar, Senegal.
4Hospital Principal Dakar, Dakar, Senegal.
*Correspondence:
Momar Dioum, Fann University Hospital Cardiology Department, Dakar, Senegal, Tel: 00221776551883.
Received: 24 Jan 2023; Accepted: 28 Feb 2023; Published: 05 Mar 2023
Citation: Momar Dioum, Papa Guirane Ndiaye, Louise Héléne Ndiaye, et al. Epidemiological, Diagnostic, Therapeutic and Evolutionary Aspects of Late-Presenting St Segment Elevation Myocardial Infarction (STEMI): About 50 Cases Collected in Four Cardiology Departments in Dakar. Cardiol Vasc Res. 2023; 7(2): 1-4.
Abstract
Introduction: The management of ST Segment Elevation Myocardial Infarction (STEMI) in African environment is a real problem with many diagnostic and therapeutic delays. The objective of this study was to identify the factors that lengthen consultation times and to assess the overall management of patients received after the deadline.
Methodology: This was a multicentre, prospective, analytical and descriptive study from August 1st, 2021 to April 30th, 2022. Were included all patients with STEMI received after the 12th hour after the onset of pain in four cardiology centers in Dakar.
Results: Fifty patients were included, representing 11.21% of all the STEMI. The predominance was male (68%). The average age of patients was 56.74 years. The main risk factors identified were hypertension (46%), diabetes (42%), dyslipidemia (36%) and smoking (34%). Chest pain was the main symptom and occurred mainly between 8h and 22h in 72% of cases. The average time between pain onset and admission to cardiology was 134.22 hours. The reasons cited for the delay in consultation were related to the late onset of pain (32%), self-medication (28%), financial concern (20%), ignorance of severity (10%) and the fact that pain is tolerable (10%). The average time between first medical contact and ECG completion was 52.64 minutes. Coronary angiography in 35 patients (70%) had mostly triple-vessel disease (28%). PCI was done in 42% of patients. Overall, the evolution was favourable (88%). Two deaths were recorded during hospitalization, for a hospital mortality rate of 4%.
Conclusion: Delays in the diagnosis and management of STEMI are enormous with significant consequences. For a definitive solution to the various factors identified, it will be necessary to change the paradigm that will mainly involve awareness and communication and the creation of a coronary pathway
Keywords
Introduction
ST Segment Elevation Myocardial Infarction (STEMI) is the ultimate stage in the evolution of coronary disease with its severe consequences in terms of morbidity and mortality [1,2]. It is often secondary to thrombotic coronary occlusion that requires rapid myocardial reperfusion, ideally within the first 12 hours, either by thrombolysis or by gold standard percutaneous coronary intervention (PCI) [3,4]. The achievement of this reperfusion in time poses many problems in our regions with many more patients received after the 12th hour defining the late-presenting STEMI.
The main objective of this study was to evaluate the overall management of patients received after the deadline and the specific objectives were to study the socio-demographic profile of patients, to describe the factors that lengthen the consultation times, the therapeutic strategy adopted and to appreciate the morbidity and mortality during hospitalization.
Methodology
This was a multicentre, prospective, analytical and descriptive study from August 1st, 2021, to April 30th, 2022, a period of 9 months.
The study had included all patients with STEMI received after the 12th hour after the onset of pain in four cardiology departments in Dakar (Aristide Le Dantec Hospital, Dakar Main Hospital, General Idrissa Pouye Hospital, and Fann National University Hospital) during the study period. Patients who refused to participate in the study and those with incomplete records were excluded.
We analyzed the epidemiological data, the management times (the delay between pain and first medical contact, the delay between the first medical contact and the first ECG, the delay between pain and admission inn cardiology), medical history and cardiovascular risk factors. Clinical data (chest pain, dyspnea and other signs) as well as paraclinical data such as electrocardiogram, biology and echocardiography data have been reported. Coronary angiography’s data were also evaluated and a record of clinical progression during hospitalization was made.
The data were entered using the SPHINX DEMO V software and the analysis carried out using the SPSS (Statistical Package for Social Science) software version 20.0.
Results
Fifty patients were included, representing 11.21% of the STEMI during this period. The predominance was male (68%). The average age of patients was 56.74 years with extremes of 22 and 85 years. The enrolment rate was 80%, the majority had secondary and university education (32%) respectively. Most had a medium socio-economic level (48%). Most patients lived in urban areas at 80 %. Personal cardiovascular history was represented by coronary artery disease (4.3%) and peripheral arterial disease (2%). The main risk factors identified were hypertension (46%), diabetes (42%), dyslipidemia (36%) and smoking (34%).
Chest pain was the main symptom and was typical in 90%. It occurred mainly between 8h and 22h in 72% of cases. The average time between onset of pain and admission to the cardiac department was 134.22 hours with a minimum of 12 hours and a maximum of 792 hours. The reasons reported for the delay in consultation were related to the late onset of pain (32%), self-medication (28%), financial concern (20%), ignorance of severity (10%) and the fact that pain is tolerable (10%). Figure 1 shows the causes of consultation delays. Patients consulted between one (78%), two (16%) and three (6%) health facilities before being admitted to cardiology. Ambulance was the most common means of patient transfer (60%); she was medicalized 32% of the time. The average time between first medical contact and ECG completion was 52.64 minutes. Clinical features are shown in Table 1. Physical examination was normal in 80% of patients. Signs of left heart failure were noted in 20% of patients.
Table 1: Patient Clinical Data.
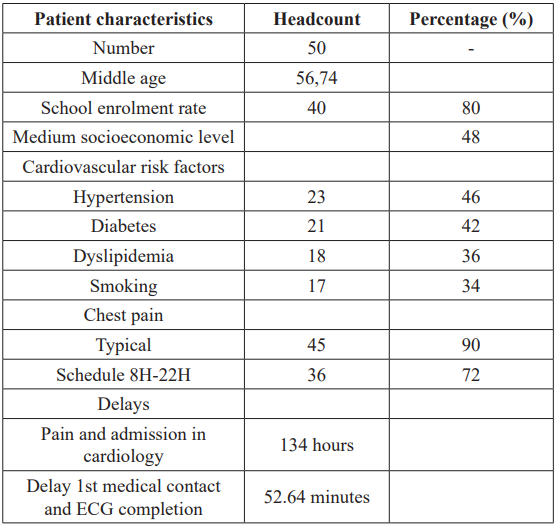
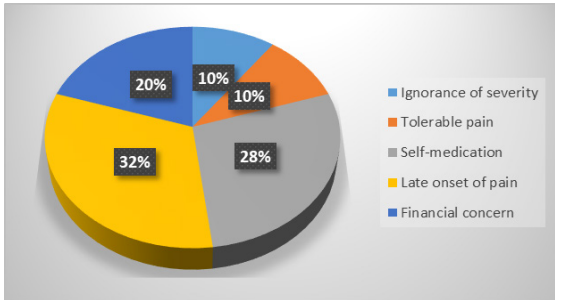
Figure 1: Causes of late consultation.
Troponinemia was positive for all patients. The electrocardiogram showed lesion of anterior territory in (66%) cases, inferior territory (28%) and lateral territory (6%). A necrosis Q-wave was present in 42 patients (84%). Rhythm and conduction disorders were present in 10 and 14% of cases respectively. Echocardiography had indicated wall motion abnormalities kinetics in 34 patients (68%). Left ventricle systolic function was impaired in 35 patients (70%). Left intraventricular thrombus was observed in 05 patients (10%) and pericardial effusion in 02 patients (4%). Coronary angiography was made in 35 patients (70%) and found one- vessel lesion in 9 patients (18%), two-vessel lesions in 11 patients (22%) and three-vessel lesions in 14 patients (28%). Left anterior descending (LAD) artery was the most affected in 37% of cases. Twenty-one patients (42% of the total population and 60% of those who received coronary angiography) had PCI. The result was good in 81% of cases. A ventricular tachycardia complication was noted per procedure in a patient.
Overall, the outcome was favorable (88%). The average length of hospitalization was 07 days. Sixteen patients (32%) had enrolled in the cardiac rehabilitation program. We noted two cases of death, a hospital mortality rate of 4%.
Discussion
As everyone knows, The management of the STEMI is a race against the clock. The goal of the treatment is to ensure the reperfusion of the guilty artery within the first 12 hours [3,4]. Better current guidelines (American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines) recommend that patients be treated primarily with PCI within 90 minutes of first medical contact (FMC) for patients who initially arrive at an hospital capable of performing angioplasty and within 120 minutes for a non-compatible hospital [5]. Knowing this disease with its high mortality and morbidity consequences [6,7], this approach to managing patients in strict time frames was associated with better patient survival [8,9]. Paradoxically, one thing was found in sub-Saharan Africa, the management of patients with STEMI was associated with very long delays with most patients who come out of time. In our series, the average time between pain onset and admission to the cardiology department was 134.22 hours and the average time between first medical contact and ECG completion was 52.64 minutes. These long delays have been found in most previous studies [10-12]. The rate of revascularization of patients by PCI was considered very insufficient at 42%.
The consequences of this delay in diagnosis and suboptimal management are not negligible with an alteration of the ejection fraction of the left ventricle noted in 70% of patients and a mortality rate of 4%.
In view of these consequences, it is important to improve diagnostic and management times. This may be achieved through a well-organized coronary care network and population awareness of coronary disease as it has been demonstrated in previous studies that the non-recognition of cardiac symptoms (44.6%) and misinterpretation of symptoms as non-serious (36.9%) were the main factors associated with delay [13,14].
Conclusion
Delays in the diagnosis and management of STEMI are enormous with significant consequences. For a definitive solution to the various factors identified, it will be necessary to change the paradigm that will mainly involve awareness and communication and the creation of a coronary pathway.
References
- Okrainec K, Banerjee DK, Eisenberg Coronary artery disease in the developing world. Am Heart J. 2004; 148: 7-15.
- Touze Les maladies cardiovasculaires et la transition épidémiologique du monde tropical. Med Trop. 2007; 67: 541-542.
- Kushner FG, Hand M, Smith Jr SC, et al. 2009 Focused Updates: ACC/AHA Guidelines for the management of patients with ST Elevation myocardial infarction (Updating the 2004 Guideline and 2007 Focused Update) and ACC/AHA/SCAI Guidelines on Percutaneous Coronary Intervention (Updating the 2005 Guideline and 2007 Focused Update): A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2009; 54: 2205-2241.
- Akoudad H, Lahlou L’angioplastie primaire à la phase aiguë de l’infarctus du myocarde. Morrocan J Cardiol. 2010: 17-24.
- O’Gara PT, Kushner FG, Ascheim DD, et al. ACCF / AHA guideline for the management of ST-elevation myocardial infarction: executive summary: a report of the American College of Cardiology Foundation / American Heart Association Task Force on Practice Guidelines. J Am Coll 29 janvier. 2013; 61: 485-510.
- De Luca G, Suryapranata H, Zijlstra F, et Temps dapparition des symptômes au ballonnet et mortalité chez les patients atteints d’infarctus aigu du myocarde traités par angioplastie primaire. J Am Coll Cardiol. 2003; 42: 991-997.
- De Luca G, Suryapranata H, Ottervanger JP, et al. Délai de traitement et mortalité dans l’angioplastie primaire pour infarctus aigu du myocarde : chaque minute de retard Circulation. 2004; 109: 1223-1225.
- Cannon CP, Gibson CM, Lambrew CT, et al. Relation entre le temps d’apparition des symptômes et le temps de porte au ballonnet avec la mortalité chez les patients subissant une angioplastie pour infarctus aigu du myocarde. JAMA. 2000; 283: 2941-2947.
- McNamara RL, Wang Y, Herrin J, et al. Effet du temps porte- ballon sur la mortalité chez les patients atteints d’infarctus du myocarde avec élévation du segment ST. J Am Coll Cardiol. 2006; 47: 2180-2186.
- Mouhamed Cherif Mboup, Maboury Diao, Khadidiatou Dia, et Les syndromes coronaires aigus à Dakar: aspects cliniques, thérapeutiques et évolutifs. The Pan African Medical Journal. 2014; 19: 126.
- Nobila Valentin Yameogo, André Samadoulougou, Georges Millogo, et Délais de prise en charge des syndromes coronariens aigus avec sus-décalage du segment ST à Ouagadougou et facteurs associés à un allongement de ces délais: étude transversale à propos de 43 cas colligés au CHU- Yalgado Ouédraogo. The Pan African Medical Journal. 2012; 13: 90.
- Mingou J, Ndiaye PG, Dioum M, et Acute coronary syndromes with persistent ST-elevation in young patients at Principal Hospital of Dakar: Epidemiological, clinical, paraclinical, therapeutic and evolutionary aspects. A report of 13 cases. Tropical Cardiology. 2021.
- Khan A, Phadke M, Lokhandwala YY, et Une étude des schémas de retard préhospitalier dans l’infarctus aigu du myocarde dans un institut de soins tertiaires urbains à Mumbai. J Assoc Physicians Inde. 2017; 65: 24-27.
- Choudhary R, Sharma SM, Kumar V, et al. Une étude observationnelle du retard préhospitalier et hospitalier dans la reperfusion pour l’infarctus aigu du myocarde dans un hôpital universitaire en Inde. J Pract Cardiovasc Sci. 2016; 2: 163- 168.