Feeding Practices and Stunted Growth in Children Aged 0-59 Months in Sedhiou
Author'(s): Sow Djiby1, Maty-Diagne-Camara2, Nafy Ndiaye3, Mouhamed Yakham LEYE4, Malang Dabo5, Ndour Michel Assane6, Faye Fulgence A7, Fall Ndiouga8, Dieng Mouhamed9, Djiba Boundia10, Diédhiou Demba11, Saou Houleye12, Diallo IM13, Sarr Anna14, Ndour Mbaye Maimouna15, Abdoulaye Leye16
Specialist in Internal Medicine, Endocrinology and Diabetology Clinique Médicale II, Centre Hospitalier Abass Ndao Cheikh Anta DIOP University, Dakar.
*Correspondence:
Dr. Djiby SOW Maitre, Assistant, Specialist in Internal Medicine, Endocrinology and Diabetology Clinique Médicale II, Centre Hospitalier Abass Ndao Cheikh Anta DIOP University, Dakar.
Received: 01 Apr 2024 Accepted: 13 May 2024
Citation: Sow Djiby, Maty-Diagne-Camara, Nafy Ndiaye, et al. Feeding Practices and Stunted Growth in Children Aged 0-59 Months in Sedhiou. Diabetes Complications. 2024; 8(2); 1-6.
Abstract
Introduction: Dietary practices can lead to stunted growth in children. The aim was to study stunting and dietary practices in children under 5 in the Sédhiou region.
Methodology: This was a descriptive and analytical cross-sectional study. The target population was children under 5 years of age. The sampling method was two-stage cluster sampling. The study period was from January 28 to February 20, 2019. Data analysis was performed using R Studio, ENA FOR SMART and Excel.
Results: A total of 748 children were colligated. The mean age of the children was 28.83 months, with a standard deviation of 15.93 months. The minimum age was 0 months and the maximum 59.53 months. The minimum height was 38.7 cm and the maximum 127.7 cm, with a median of 83.9 cm. Males accounted for 51.2%, with a sex ratio of 1.04 in favor of males. The overall prevalence of chronic malnutrition in children aged 0-5 years was 29.7%. Bivariate analysis showed that breastfeeding (p=0.01), colostrum administration (p=0.02) and parents' level of education (p=0.02) were significantly associated with stunted growth in children. Multivariate analysis showed that the main factor associated with stunted growth in children aged 0 to 5 in Sédhiou was breastfeeding (p=0.016).
Conclusion: In Sédhiou, breastfeeding, the administration of colostrum and parents' low level of education are explanatory factors for chronic malnutrition in children under 5. A wide-ranging communication campaign would raise parents' awareness of the importance of exclusive breastfeeding for children's health.
Keywords
Introduction
Good nutrition is essential for a child's development: worldwide, 60% of infant and young child deaths are due to inappropriate feeding practices and infectious diseases, two-thirds of which are attributable to inadequate breastfeeding practices [1]. In developing countries, malnutrition is the underlying cause of more than 50% of deaths in children under 5 years of age [2]. Inappropriate feeding practices play a key role in the genesis of this condition. In developing countries, feeding practices are very often inadequate and incompatible with the recommendations of the World Health Organization (WHO), and are the main factors affecting children's physical growth and mental development [3,4]. In 2017 in Senegal, 16.5% of children under 5 years of age and 19% in 2019 suffer from chronic malnutrition [5]. Moreover, in the Sédhiou region, despite the availability of health structures and the existence of numerous nutritional potentialities, the prevalence of chronic malnutrition remains precarious, being 29.6% in 2018 and 28.7% in 2019 [6,7]. However, there are very few specific studies on chronic malnutrition in children under 5 in Senegal.
This motivates us to carry out this study in order to see the share of dietary practices on stunting in children under 5 in Sedhiou in 2019.
Patients and Methods
Study framework
The Sédhiou region covers an area of 7,330 km², or 3.7% of the national territory. The population of the Sédhiou region is estimated at 55,3005 inhabitants (Agence Nationale de la Statistique et de la Démographie 2019) with a density of 76 inhabitants per Km² with women of reproductive age (129,173) and 0-59 months numbering 88,058 children. The medical region is made up of 3 health districts.
Survey type
This was a stratified, quantitative sample survey,
Defining the target population
The target population for the survey was children under 5 years of age. Infant and young child feeding (ANJE) covered children aged 0-23 months.
Inclusion criteria
In each selected household, all children aged 0-59 months were included in the survey, as well as all women aged 15-49.
Non-inclusion criteria
Refusals and children who were ill on the day of the survey were not included in the study.
Sampling protocol
The sampling method chosen for this survey was a systematic two-stage cluster random sampling. Stratification was carried out at regional level for individual indicators (nutrition), and at departmental level and by area of residence for household indicators (food security and resilience). The selection of RDs was carried out by systematic random sampling based on probability proportional to the population size of the primary sampling units (RDs). The second stage of sampling involved the selection of households within the sampled PDs. Household selection was carried out using the systematic random method, applying a sampling step (P) which is the number of households separating two sampled households. The step size in each RD is calculated by dividing the number of households (N) in the RD by the number of households to be surveyed (n). The number obtained by this operation is the sampling step used to select the households in the sample.
Sample size calculation
It is carried out using the ENA for SMART software version of July 09, 2015. In the Sédhiou region, the sample size is 537 households for 34 DRs.
Operational definition of variables to be collected
• Anthropometry and children's health
Sex: The sex variable was collected and coded "m" for male and "f" for female
Age: The date of birth of eligible children was collected from official documents (birth certificate, suppletive judgment, health record), or age was estimated using the local events calendar.
Height: Height was measured using a SHORR measuring tape graduated in centimetres and accurate to the nearest millimetre. Children under 24 months were measured lying down, and those 24 months and over standing up.
Coverage of vitamin A supplementation and deworming Vitamin A supplementation: This information was collected from children aged 6 to 59 The aim was to find out whether the child had received vitamin A supplementation in the last 6 months.
Deworming of children: this information was collected from children aged 12 to 59 months. The aim was to find out whether the child had been dewormed in the last 6 months.
Feeding practices for children aged 0 to 23 months Information on infant and young child feeding practices was collected by administering a series of questions to the mother or guardian to assess current feeding practices in children under 24 months of age.
Exclusive breastfeeding
Proportion of infants aged 0-6 months exclusively breastfed.
Continued breastfeeding at one year
Proportion of children aged 12 to 15 months who are breastfed.
Continued breastfeeding up to 2 years and beyond
Proportion of children aged 20 to 23 months who are breastfed.
Data collection method
Data were collected over the period from January 28 to February 20, 2019, using standardized questionnaires based on SMART, WHO and FANTA 2 recommendations1 . These questionnaires were converted into an electronic version that could be downloaded onto tablets using the Android operating system.
Data collection was carried out on the tablets using the Sapmobil version 1.6v application developed in WLanguage and JAVA.
Data analysis method Analysis method
Data were analyzed using R studio and ENA FOR SMART software. The risk of error being equal to 5%, the significance threshold was p < 0.05.
Descriptive analysis
The first step was to describe the various quantitative and qualitative variables collected in terms of positional parameters (means, median, frequencies) and dispersion parameters (extremes, standard deviation).
To determine the nutritional status of children under 5, we used the Z-score, which is a measure of the stunting index. It is calculated as follows:
Z-Score Size/Age = Te-Tm / ET where:
Te = Height of the child, Tm = Median height in the reference population (for the age and sex of the child in question), SD= Standard deviation in the reference population.
Children between the standard deviations of -2 and -3 (-3 < Z Score < -2) are considered moderately malnourished, while those below the standard deviation of -3 (Z Score < -3) are considered severely malnourished.
Bivariate analysis
The second step was bi-variate analysis. The Chi2 or Fischer test was used to compare two qualitative variables. It is significant when p is less than 0.05.
Multivariate analysis
To explain the factors associated with stunted growth in children, we used a logistic regression model in which we included all the variables that in bivariate analysis had a p<0.25, and we performed a stepwise descending regression.
Study limits
Despite the high response rate, there were a number of missing data relating to the variables of research interest. As a result, the database was adjusted by deleting any households, children or variables for which multiple responses were missing. In the end, the final sample used consisted of 518 households.
The variables: early breastfeeding and colostrum are not included in the multivariate analysis, despite the fact that there is a statistically significant link between stunted growth and these variables. For the variable early breastfeeding, the proportion of non-respondents was over 50%. We therefore decided not to include it in the basic model. There was also no variable to explain the reasons for non-response (i.e. whether the mother was ill or died after delivery). For the colostrum variable, its presence in the basic model means that variables that were highly significant in the bivariate analysis become insignificant once again.
Ethical considerations
Parental consent was obtained orally. We obtained the agreement of the health authorities of the Abobo West health district and of the community leaders of Anonkoi3. The electronic data file was anonymous.
Results
Epidemiological characteristics
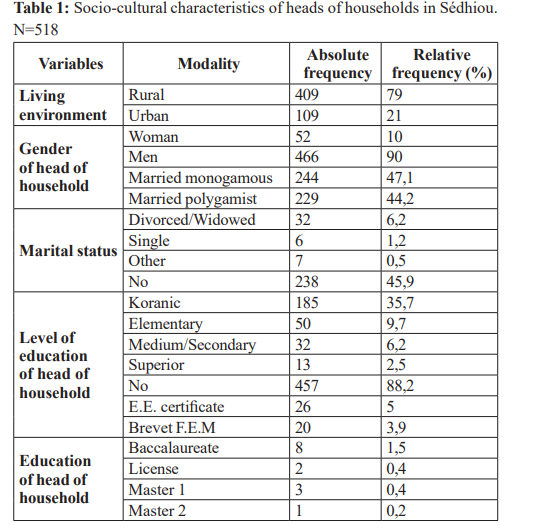
During the study, 748 cases were colligated. Males accounted for 51.2%, with an m/f sex ratio of 1.04. The mean age of the children was 28.83 months, with extremes ranging from 0 months to 59.53 months. The mean height of the children was 83.9 cm, with a standard deviation of 14.17 cm. The minimum height was 38.7 cm and the maximum 127.7 cm, with a median of 83.9 cm. The majority of children (79%) lived in rural households and 21% in urban ones. The majority of heads of household were men (90%), with a sex ratio of 8.96. The school enrolment rate among heads of household was 18.4%, with 9.7% in primary school, 6.2% in middle/secondary school and 2.5% in higher education. Those who have attended Koranic school represent 35.7%. The majority of heads of household (88.2%) have no formal education. Only 5% have an elementary school certificate and 0.2% a Master 2 (Table 1).
Children's eating habits
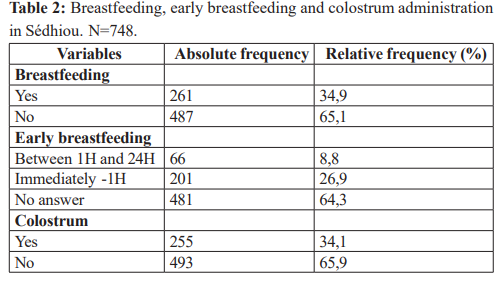
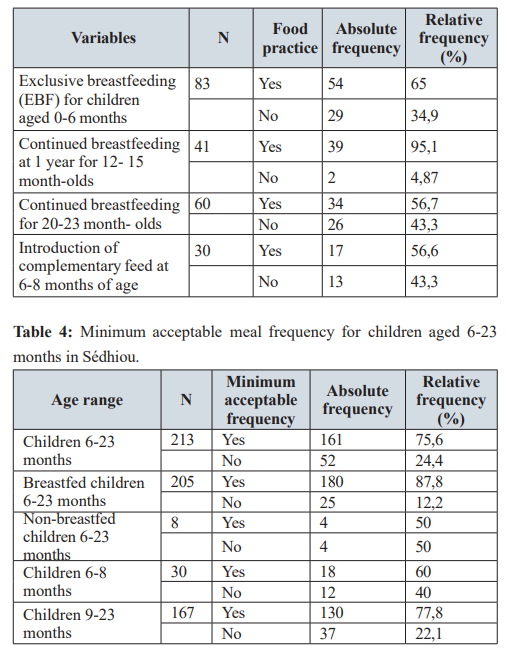
Only 35.1% of children aged 12-59 months are dewormed in urban areas, compared with 64.9% in rural areas. And 31.7% of children aged 6-59 months are supplemented with vitamin A in urban areas versus 68.3% in rural areas. There was a statistically significant relationship between place of residence and vitamin A supplementation (p= 0.004). No statistically significant relationship was found between place of residence and deworming (p=0.102). Only 33.5% of children aged 6- 59 months received vitamin A supplementation, and 29.2% of children aged 12-59 months were dewormed. The results show that only 34.9% of children are breastfed. For early breastfeeding, 26.9% of children were immediately put to the breast. The majority of children (65.9%) were not given colostrum at birth. Sixty-five percent (65%) of children aged 0-6 months were exclusively breastfed. Breastfeeding continued for up to 1 year in 95.1% of children. Some 56.7% of children continued to receive breast milk up to 2 years. The introduction of complementary foods was observed in 56% of children (Table 2).
Minimal dietary diversity in children aged 6-23 months
More than half (75.8%) of children consumed fewer than 4 food groups the day before the survey. The results reveal that 78.4% of breast-fed children and 75% of non-breast-fed children do not have a diverse diet the minimum meal frequency for children aged 6-23 months is 75.6%. This is higher for breastfed children (87.8%) than for non-breastfed children (50%). Table 3 shows that 60% of children aged 6-8 months and 77.8% of children aged 9-23 months have the minimum frequency of meals recommended for their age. Table 4 shows that the proportion of breastfed children aged 6-23 months who have a minimum acceptable diet is 21.22%. All non- breastfed children (100%) do not have a minimum acceptable diet.
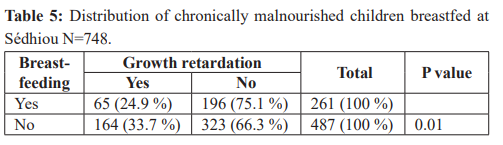
The overall prevalence of chronic malnutrition is 29.7%, with 30.4% among boys and 29% among girls. The moderate form is 18.5%, with 19.2% among girls and 17.7% among boys. And the severe form is 11.2%, with 12.6% in boys and 9.7% in girls. The prevalence of stunting is 33.7% in children who are not breastfed, compared with 24.9% in those who are. There was a statistically significant relationship between stunting and breastfeeding (p=0.01).
33.3% of chronically malnourished children did not receive colostrum at birth, compared with 25.5% of those who did. There was a statistically significant relationship between growth retardation and colostrum administration (p=0.02). Thus, 24.1% of exclusively breastfed children were stunted, compared with 27.6% of those who were not. There was no statistically significant relationship between chronic malnutrition and exclusive breastfeeding (p=0.72), and the prevalence of stunting was 44.1% among children breastfed for up to 2 years, versus 26.9% for those not breastfed. There was no statistically significant relationship between chronic malnutrition and continued breastfeeding at age 2 (p=0.17) (Table 5). 31.2% of children with acceptable dietary diversity were stunted, compared with 20.4% of those without. There was no statistically significant relationship between stunting and dietary diversity (p=0.11).The results showed that 25.6% of children who had a minimum meal frequency were stunted, compared with 15.6% of those who did not have the minimum acceptable frequency. There was no statistically significant relationship between chronic malnutrition and minimum meal frequency (p=0.15). The results show that minimum acceptable frequency (60.1%) and dietary diversity (63.8%) are higher in rural than in urban areas. However, this difference was not statistically significant (p=0.28; p=0.34).
Discussion
The overall prevalence of chronic malnutrition is 29.7%, with 30.4% among boys and 29% among girls. In Côte d'Ivoire, it was 22.5% [8]. In Mali, SANGHO O et al. found a prevalence of 14% for acute malnutrition, of which 4.4% was severe [9]. In our study, the severe form was 12.6% in boys and 9.7% in girls. In our study, malnutrition affected boys more than girls. In Mali, it was more prevalent among females (51%) [9], and the prevalence of stunting was 33.7%. According to the WHO, 155 million children under the age of five are stunted, while 41 million are overweight [1]. In West and Central Africa, around 40% of children under 5 are stunted, and 60% are anemic [10].In Benin, the prevalence was 53% of children surveyed were stunted [11].This high prevalence can be explained by the fact that the majority of children (65.1%) were not breastfed. Multivariate analysis showed that children who were not breastfed were 1.54 times more likely to suffer from chronic malnutrition than those who were breastfed [1.08, 2.19], with a (p= 0.016).on the other hand, early breastfeeding was only noted in 26.9%. Thus, for early breastfeeding after birth, the rate was very low compared with the national level of 53.9% [12].Feeding practices are the determining factors in children's nutritional status, which in turn affects morbidity and mortality.
As far as breastfeeding is concerned, it should be noted that breast milk contains all the nutrients children need in the first few months of life, and helps avoid nutritional deficiencies [13].
Indeed, exclusive breastfeeding is the best option for infant feeding [14]. The present study shows that the majority of children (65%) were exclusively breastfed in Sédhiou.
Since 2001, the WHO has recommended exclusive breastfeeding (EBF) for up to six months and partial breastfeeding for up to two years [3]. This is the optimal way to feed newborns. In one study, exclusive breastfeeding was practised by only 30.66% of those surveyed. It was continued 'at 24 months in only 29% [15].
However, breastfeeding within 30 minutes of delivery has been shown to have a beneficial effect on the duration of breastfeeding [16]. Al ghwass et al. in Egypt even recommended that breastfeeding within the first hour of delivery led to a 2-fold increase in the likelihood of AME [17]. However, our results show that there is no statistically significant link between stunting and exclusive breastfeeding (p=0.72). In sum, reinforcement actions are needed to reach a prevalence of exclusive breastfeeding above 90% to prevent malnutrition and considerably reduce the risk of infectious diseases such as diarrhea and pneumonia. They were present in 12.7% and 17.8% of children respectively in the last two weeks before the survey. However, from the age of six months, the baby must receive complementary foods in addition to breastfeeding, which must continue until the age of 2 or beyond. Our results show that more than half of infants aged 6 to 8 months received solid, semi-solid or soft foods. However, there was no statistically significant relationship between growth retardation and the introduction of complementary foods (p=0.56). These feeding practices require mothers to learn how to prepare food properly, in order to avoid diarrhoeal illnesses and also to avoid abandoning breastfeeding. In favor of liquids and porridge. It has also been shown that the late introduction of solid, semi-solid or soft foods poses a threat to growth and development [18]. Our results show that more than half (75.8%) of children aged 6-23 months do not have a diversified diet.
Our results also show that the diets of rural children are more diversified than those of urban children. But the paradox is that the prevalence of stunting is higher in children with a diversified diet. Further studies are needed to identify other factors that may explain this paradox. However, there is no statistically significant link between dietary diversity and stunting in Sédhiou. However, a varied diet enables children to consume all the essential foods their bodies need. The monotonous diet of Chadian women, consisting mainly of milk and cereals, was described in 2005 [19]. In Burkina Faso, a study showed that only a quarter of children aged between 6 and 23 months had a minimum dietary diversity [20]. For some authors, there is a positive relationship between household economic situation and high dietary diversity [21].
In this study, it was found that the majority of children aged 6-23 months ate all three meals as recommended. This was higher in rural areas (60.1%) than in urban areas (39.9%). Nevertheless, the results show that stunted growth is more prevalent among those who eat at the minimum acceptable frequency. But there was no statistically significant relationship between minimum acceptable frequency and chronic malnutrition (p= 0.15). Elsewhere, the minimum meal frequency was 60.1% for all children [20].
To improve children's nutritional status, the Senegalese government has initiated several strategies, such as vitamin A supplementation and deworming. However, our results show that only 33.5% of children are supplemented with vitamin A in Sédhiou, compared with 59.2% nationally [12].
Supplementation was more common in rural children (68.3%) than in urban children (31.7%). This difference is statistically significant (p=0.015). However, there was no statistically significant link between stunted growth and vitamin A supplementation. It should be noted that inadequate vitamin A intake can increase the risk of morbidity and mortality from childhood infections such as measles and diarrhoeal diseases. This is demonstrated by Imdad A et al., in 2017, that vitamin A supplementation is associated with a reduction in morbidity and mortality in children [22]. This justifies all the interest of the national protocol for the management of acute malnutrition, which recommends that every child aged 6 months be supplemented with vitamin A [23].
Our study shows that only 29.2% of children are dewormed. Deworming combats intestinal worms, reduces the risk of anaemia and promotes rapid weight and height recovery [22]. This is why the national protocol for the management of acute malnutrition recommends that all children aged 12 months should be dewormed and rewormed every six (6) months [23].
References
- Global Strategy for Infant and Young Child Feeding. WHO.
- Levels and trendsin child malnutrition Joint child malnutrition estimates. WHO. 2015.
- Mukuku OK, Mutombo AM, Lubala TK, et al. Predictive score of severe acute malnutrition in children under 5 years in developing countries development and validation. Trop Med Int Health. 2015; 20: 80.
- Report of the expert consultation on the optimal duration of exclusive breastfeeding. WHO. 2001.
- Agence nationale de la statistique et de la démographie. Enquête Démographique et de Santé ANSD. 2017.
- Cellule de lutte contre la Senegals multisectoral nutrition strategic plan.
- Executive Secretariat of the National Food Security Council. SECNSA. 2019.
- Sackou Kouakou JG, Aka BS, Hounsa AE, et Médecine et Sante Tropicales. 2016; 26: 312-317.
- Sangho O, Doumbia A, Samake A, et al. Prevalence of acute malnutrition in children aged 6-59 months in the health district of Barouéli. Mali Sante Publique. 2013; 3: 00176.
- Sibiri Bougma, Franck Garanet, Aly Savadogo, et al. Factors associated with growth retardation in a context of food supplementation in Burkina Faso. Cahiers de Nutrition et de Diététique. 2019; 54: 108-115.
- Yessoufou A, Ahokpe M, Behanzin j, et al. Prevalence de la malnutrition aigue chez les enfants de moins de cinq ans dans la plaine de pendjari au nordouest du benin. J rech sci univ lomé. 2014; 16: 69-78.
- Executive Secretariat of the National Food Security Council. SECNSA. 2019.
- Enquête Démographique et de Santé Continue. 2015.
- Evolution de la prévalence de la malnutrition chronique et de ses déterminants chez les enfants de moins de cinq ans au Niger. NiPN. 2019; 30.
- Mahamadou Traoré, Hamadoun Sangho, Maty Camara Diagne, et al. Fnta Sangho Factors associated with exclusive breastfeeding among mothers of 24-month-old children in Bamako. In Santé Publique. 2014; 26: 259-265.
- Peters E, Wehkamp KH, Felberbaum RE, et Breastfeedind duration is determined by only a few factors. Eur J Public Health. 2006; 16: 162-167.
- Al Ghwass MM, Ahmed Prevalence and predictor of 6-month exclusive breastfeeding in a rural area in Egypt. Breast feeding Med. 2011; 6: 191-195.
- From the first hour of life Advocacy to improve infant and young child feeding worldwide. Unicef. 2016; 104.
- Schelling E, Daoud S, Daugla DM, et al. Morbidity and nutrition patterns of three nomadic pastoralist communities of Chad. Acta Trop. 2005; 95: 16-25.
- Bougma Sibiri, Hamaba Fatoumata, Garanet Franck, et al. Caracteristiques sociodemographiques des meres et pratiques dalimentation de complémentaire chez les enfants de 6 a 23 mois dans le centre nord du Burkina Faso. Afr J Food Agric Nutr Dev. 2022; 22: 22017-22040.
- Ilana N Bezerra, Rosely Sichieri. Household food diversity and nutritional status among adults in Int J Behav Nutr Phys Act. 2011; 8: 22.
- Imdad A, Mayo WE, Herzer K, et Vitamin a supplementation for preventing morbidity and mortality in children from six months to five years of age. Cochrane Database Syst Rev. 2017; 3: CD008524.
- Protocole national de prise en charge de la malnutrition aigüe. MSAS-DAN. 2013.