Prevalence and Profile of Anemia in Diabetic Patients in Nouakchott, Mauritania: An Observational Study
Author(s): Ghaber Sidi Mohamed1,2*, Tfeil Yahya1,2, Mohamed Jiddou Sidi Baba1,2, Meiloud, Ghlana1, Lella Mohamed Lemine1,3, Dahiya Mohamed1,2, and Ould El Kebir MV1
1Food, Nutrition, and Metabolic Disorders Research Unit - FST - University of Nouakchott, Mauritania.
2Faculty of Medicine, University of Nouakchott.
3Department of Diabetology and Endocrinology, National Hospital of Nouakchott, Mauritania.
*Correspondence:
Ghaber SM, Food, Nutrition, and Metabolic Disorders Research Unit - FST - University of Nouakchott, Mauritania.
Received: 10 Feb 2024 Accepted: 18 Mar 2024
Citation: Ghaber SM, Yahya T, Jiddou SBM, et al. Prevalence and Profile of Anemia in Diabetic Patients in Nouakchott, Mauritania: An Observational Study. Diabetes Complications. 2024; 8(2); 1-5.
Abstract
This observational and descriptive study examined the prevalence of anemia among a cohort of 1073 diabetic patients residing in Nouakchott, Mauritania. It also explored the complex interactions between anemia, diabetes, and chronic kidney disease (CKD), while analyzing variations based on gender, age, and ethnic origin.
The results reveal a prevalence of anemia reaching 13.4% within the study population. Most cases were characterized by mild anemia, followed closely by moderate anemia, while cases of severe anemia were rare. Furthermore, it is important to note that most cases of mild and moderate anemia were associated with relatively normal kidney function. Demographically, women, with an average age of 55, were three times more affected by anemia than men, who had an average age of 61. The highest prevalence of anemia were observed in women aged 41 to 50 and in men aged 51 to 60. Ethnic data also revealed that Moors constituted the majority of anemia-affected patients, accounting for 76.4%, while Blacks represent only 23.6% of this population. These findings highlight the importance of closely monitoring anemia in diabetic patients, especially in women and specific ethnic groups. They also underscore the complexity of the relationships between anemia, diabetes, and CKD, paving the way for future research to better understand these interactions and enhance the management of these patients.
Keywords
Introduction
Diabetes is a major global health issue, affecting millions of people worldwide. In addition to well-documented complications such as cardiovascular problems, diabetes is also linked to other medical conditions, including anemia and chronic kidney disease (CKD). Anemia, characterized by a reduction in the number of red blood cells or hemoglobin in the blood, can have a significant impact on the health and quality of life of diabetic patients. Furthermore, CKD is frequently observed in individuals with diabetes, further complicating their medical management [1-4]. Despite evidence of this association, there are variations in the prevalence of renal anemia within the diabetic population, depending on various factors, including gender and ethnicity [5-8]. However, the understanding of the interactions between diabetes, anemia, and CKD is still limited, and there is limited specific data on these relationships in our populations. It is in this context that our study was conducted, focusing on a cohort of 1072 diabetic patients residing in Nouakchott, Mauritania. The primary objective of this observational and descriptive study was to explore the prevalence of anemia within this population and determine how it interacts with diabetes and CKD.
Methods
Study Population
Voluntary diabetic patients were recruited in Nouakchott, Mauritania.
Collection of Demographic Data
Demographic information such as gender, age, and ethnicity were collected for each participating patient in the study. Data were obtained from medical records, patient interviews, or questionnaires filled out by participants.
Measurement of Hematological Characteristics
Particularly hemoglobin (Hb) levels, were measured for each patient at the MAURILAB Institute in Nouakchott, Mauritania. Blood samples were collected, and Hb levels were determined using standardized laboratory analyses.
Anemia Screening
To assess the prevalence of anemia, Hb level values were used as the screening criterion. Patients with Hb levels below a specified threshold were considered to have anemia. Measurement of CKD Progression: We assessed CKD progression by calculating creatinine clearance (eGFR origin ml/min/1.73m²) within our study population. This analysis allowed us to classify CKD into five distinct stages, ranging from "Normal Stage" to "End-Stage CKD," using standard CKD classification criteria.
Statistical Analysis
The collected data were analyzed using IBM SPSS 25. Percentages, means, and standard deviations were calculated to describe the demographic distribution, hematological characteristics, and prevalence of anemia in the study population. Statistical tests were used to assess significant differences between groups (e.g., between genders or ethnic groups).
Ethics and Consent
The study was conducted following ethical principles and applicable regulatory guidelines. Patients were informed of the study's purpose and provided informed consent before participation. Research protocols were approved by the ethics committee of the University of Nouakchott, Mauritania.
Results
Glycemic and Hematological Characteristics of the Studied Diabetic Population
Glycemic Characteristics
The minimum fasting blood glucose level in the study population was 0.39 g/L in males and 0.57 g/L in females, while the maximum fasting blood glucose level was 5.95-5.96 g/L for both sexes. Regarding glycated hemoglobin (HbA1c), the values ranged from 4.7-4.8 to 14.4-14.5 for both sexes. Furthermore, it was observed that 23.8% of the studied population had well-controlled blood glucose levels.
Hematological Characteristics of the Study Population
The minimum Hb (hemoglobin) level observed in the studied population (1072 individuals) was 5.49g/dl in males and 6.90g/ dl in females. In contrast, the maximum Hb levels were 18.30g/ dl in males and 17.00g/dl in females. The average Hb levels were 14.27g/dl for males and 12.86g/dl for females.
Prevalence of Anemia in the Studied Diabetic Population
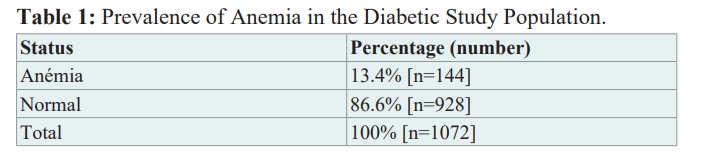
The analysis of anemia prevalence reveals (Table 1) that there were 144 cases of anemia among the participants, representing 13.4% of the total sample. The remaining 928 cases were considered normal, thus representing 86.6% of the study population.
Relationship between Diabetes, Anemia, and chronic kidney disease (CKD)
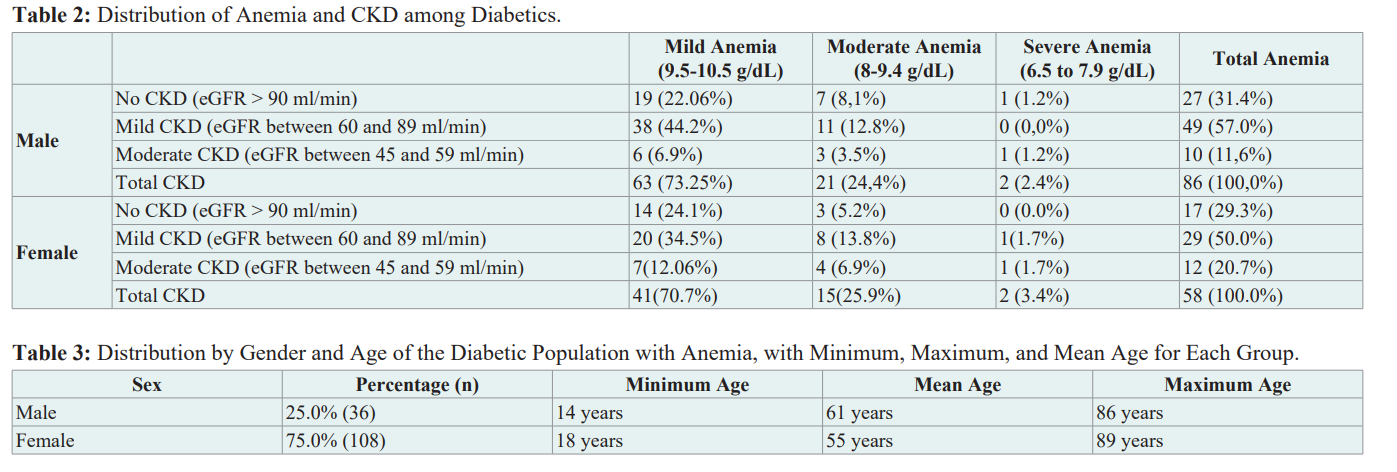
Table 2 shows that the majority of diabetics with anemia have mild anemia (73.25% in males and 70.7% in females), followed by moderate anemia (24.4% in males and 25.9% in females). Severe anemia cases are very rare (2.4% in males and 3.4% in females).
Diabetics with mild anemia (both males and females) are primarily distributed between those without CKD (eGFR > 90 ml/min) and those with mild CKD (eGFR between 60 and 89 ml/min), accounting for 22.06% and 44.2% in males, respectively, and 24.1% and 34.5% in females. This suggests that most cases of mild anemia are associated with relatively normal kidney function. Cases of moderate anemia are also distributed between those without CKD and those with mild CKD, although the proportion of mild CKD is higher (12.8% and 13.8% compared to 8.1% and 5.2%, respectively, in males and females). This indicates that moderate anemia is also frequently associated with relatively preserved kidney function. Severe anemia cases are rare but can be found in the categories of mild and moderate CKD. No cases of anemia are associated with severe or end-stage CKD in this sample.
Distribution of Diabetic Population with Anemia by Gender, Age, and Ethnicity
Distribution by Gender and Age of the Diabetic Population with Anemia, with Minimum, Maximum, and Mean Age for Each Group
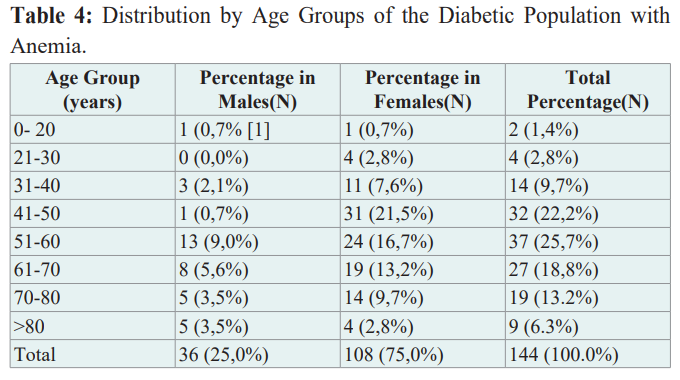
The distribution of the population with anemia in terms of gender (Table 3) indicates that 25.0% of individuals with diabetes and anemia are males, while 75.0% are females. Males had an age range from 14 years to 86 years, with a mean age of 61 years. Females, on the other hand, had an age range from 18 years to 89 years, with a mean age of 55 years.
Distribution by Age Groups of the Diabetic Population with Anemia
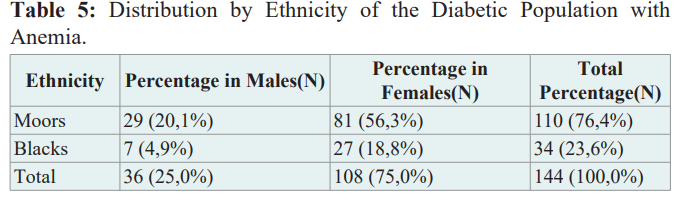
The distribution by age groups of the studied population (Table 4) highlights a significant disparity between genders regarding the prevalence of anemia. Women are significantly more affected than men in all age groups. There is a peak among women aged 41 to 50, with 31 individuals affected, representing 21.5% of all women in this category. Among men, the most affected age group is 51 to 60, with 13 individuals affected, accounting for 9% of all men in this category. In comparison, among women in the same age group, the rates of anemia are higher, with 24 individuals affected, representing 16.7% of this population. It is interesting to note that anemia rates are significantly low in men under 50 and over 70 years old. In contrast, among women, anemia rates have a low prevalence only in those under 30 or over 80 years old.
Distribution by Ethnicity of the Diabetic Population with Anemia
Data from Table 5 indicate that Moors make up 76.4%, and Blacks account for 23.6% of the total individuals with anemia. Among males, 29 belong to the Moor ethnicity, representing 20.1% of the male population studied. Regarding females, there are 81 individuals of Moor ethnicity, comprising 56.3% of the female population studied. As for the Blacks ethnicity, 7 males (4.9%) and 27 females (18.8%) belong to it.
Discussions
The prevalence of anemia, estimated at 13.4%, indicates that many individuals with diabetes also have this condition. This result is consistent with previous studies that have established a link between diabetes and an increased risk of anemia [2,9-11].
The underlying mechanisms for this association may include alterations in the production of erythropoietin, a hormone essential for red blood cell formation, as well as issues related to the absorption and regulation of iron metabolism in individuals with diabetes [1,3]. Furthermore, our study aligns with the findings of authors [10] and [12], which found that the prevalence of anemia was significantly higher in diabetic women than in diabetic men, suggesting a correlation between gender and anemia in diabetic patients. These variations in prevalence observed among different studies could be attributed to various factors such as nutrition, diet, ethnicity, and altitude, as suggested by authors [10].
It is important to note that these same authors [10] did not observe any significant difference in terms of anemia frequency between patients with type 2 diabetes and those with type 1 diabetes, suggesting that our results may be applicable to type 1 diabetes, although we did not specifically examine this population. However, they did establish a statistically significant association between anemia and chronic kidney disease (CKD), supporting our observations on the association between anemia and CKD.
Some studies also suggest that anemia is more often a consequence of diabetes complications, particularly chronic kidney disease (CKD) [13]. The results of our study note that the majority of cases of mild anemia in diabetics are associated with relatively normal kidney function, i.e., glomerular filtration rate (GFR) greater than or equal to 90 ml/min. The number of anemic patients gradually decreases with the progression of kidney disease. This finding is consistent with some previous studies that have suggested that mild anemia is often observed in diabetic patients in the early stage of chronic kidney disease, when renal function is still preserved [14,11]. One possible explanation is that diabetes itself can contribute to the development of anemia through various mechanisms, including alterations in erythropoietin production [15]. Regarding moderate anemia, it is interesting to note that although it is also present in diabetics with mild CKD, a larger proportion of these cases is observed in those with moderate CKD. This observation suggests that moderate anemia may persist or worsen with the progression of CKD. This idea is consistent with the scientific literature indicating that CKD can further disrupt erythropoietin production, leading to more severe anemia [16]. However, it is important to note that cases of severe anemia are rare in our sample, and none of them are associated with severe or end-stage CKD. This difference can be explained by the fact that patients with severe or end-stage CKD are generally managed more intensively, including erythropoietin supplementation or blood transfusions to correct anemia [17]. Finally, diabetics with mild or moderate CKD should receive special attention regarding their anemic status because even though cases of severe anemia are rare, they can occur in those with relatively preserved kidney function. Early management of anemia can have a positive impact on the quality of life and the progression of kidney disease in these patients [18]. The results of [19] also emphasize the importance of considering gender and diabetic retinopathy as risk factors associated with anemia in diabetics with moderate renal insufficiency.
The distribution of the diabetic population with anemia by sex, age, and ethnicity provides more detailed information to understand potential risk factors and differences within the studied population. Regarding the distribution by sex and age, the results show that women are significantly more affected by anemia than men, with a prevalence of 75.0% compared to 25.0%. This gender disparity is consistent with previous epidemiological studies that have shown a higher prevalence of anemia in women, in part due to menstrual blood losses and the impact of pregnancy on iron reserves [5,6]. According to different authors, these factors increase the risk of iron depletion in women, thus contributing to a higher prevalence of anemia among them.
The analysis by age groups also reveals significant variations in the prevalence of anemia in different age brackets. This relationship between anemia and age in diabetics has been highlighted [11]. Our results show a peak prevalence in women aged 41 to 50 years, which could be associated with a combination of factors, including cumulative menstrual losses and hormonal changes at this age. Among men, the age group most affected is 51 to 60 years, suggesting that specific factors related to this stage of life could also play a role in the prevalence of anemia. From an ethnic perspective, the results indicate that the Maures make up the vast majority of the diabetic population with anemia, with a prevalence of 76.4%, while Blacks represent a minority within this population, with a prevalence of 23.6%. This result is of significant importance in the context of our study. These ethnic differences in the prevalence of anemia likely reflect a diversity in access to healthcare, dietary practices, rates of nutritional deficiencies, and other socio-economic and cultural factors, all of which contribute to the risk of anemia within these ethnic groups [7,8].
However, it is also important to note the contradictory finding suggested by authors [11], which implies that the Black race is more prone to the coexistence of anemia and diabetes. This divergence underscores the complexity of the factors at play. It highlights the importance of conducting in-depth research and considering multiple variables to gain a comprehensive understanding of the relationships between anemia, diabetes, and ethnic factors. This complexity underscores the need to continue investigations to elucidate these complex interactions and better guide efforts in the prevention and management of anemia in individuals with diabetes, especially within specific ethnic groups.
Conclusion and Perspectives
In conclusion, our study has provided essential information about the prevalence of anemia among a cohort of diabetic patients in Nouakchott, Mauritania. The results have highlighted a significant prevalence of anemia, affecting nearly 13.4% of the studied population. Mild anemia was the most common form, followed closely by moderate anemia, while cases of severe anemia were rare. Furthermore, it is interesting to note that most cases of mild and moderate anemia were associated with relatively normal kidney function. Demographically, a clear disparity in prevalence was observed between genders, with women being three times more affected by anemia than men. This disparity was more pronounced in women aged 41 to 50 years and in men aged 51 to 60 years. Ethnic data also revealed that the Maures made up the vast majority of patients with anemia, while Blacks represented a smaller proportion of this population. In terms of future perspectives, the study highlights the crucial importance of monitoring anemia in diabetic patients, especially in women and within specific ethnic groups. This underscores the need for an individualized care approach that takes into account these specific risk factors. Furthermore, the study opens the door to future research perspectives. It is imperative to deepen our understanding of the complex interactions between anemia, diabetes, and chronic kidney disease by investigating the underlying mechanisms of these relationships. Longitudinal studies could help establish causal links and identify potential interventions to prevent and manage anemia in diabetic patients. Additionally, efforts should be made to raise awareness among healthcare professionals and patients about the importance of early detection and management of anemia, especially in high-risk groups. Ultimately, this study contributes to improving care for diabetic patients by highlighting an often overlooked aspect of their health, namely anemia, while emphasizing the importance of ongoing research to better understand and manage these medical complexities.
Competing interests
The authors declare that they have no competing interests.
Author contributions
All authors contributed to the conduct of this work. All authors also declare that they have read and approved the final version of the manuscript.
References
- Thomas MC, MacIsaac RJ, Tsalamandris C, et Uncontrolled Diabetes Increases the Prevalence of Anemia in Patients with Type 2 Diabetes The Fremantle Diabetes Study. Diabetes Care. 2006; 29: 752-757.
- Standards of Medical Care in Diabetes 2019. Diabetes Care. 2019; 42: S14-S80.
- Adeyemo TA, Adeleye JO, Adebisi JA, et al. Anaemia in Nigerian patients with diabetes mellitus. African Journal of Medicine and Medical 2015; 44: 165-170.
- Pehlivanoglu, Özkan. The Frequency and Some Causes of Anemia in Patients with Diabetes Mellitus with Normal Renal TJFMPC. 2020; 14.
- Kassebaum NJ, Jasrasaria R, Naghavi M, et al. A systematic analysis of global anemia burden from 1990 to 2010. Blood. 2014; 123: 615-624.
- McLean E, Cogswell M, Egli I, et al. Worldwide prevalence of anemia WHO Vitamin and Mineral Nutrition Information System 1993-2005. Public Health 2009; 12: 444-454.
- Balarajan Y, Ramakrishnan U, Özaltin, E, et al. Anaemia in low income and middle income countries. The Lancet. 2011; 378: 2123-2135.
- Suchdev. 2019.
- Abate A, Birhan W, Alemu A, et Association of anemia and renal function test among diabetes mellitus patients attending Fenote Selam Hospital West Gojam Northwest Ethiopia a cross sectional study. BMC Blood Disorders. 2013; 13: 1-7.
- Kehailou, Fatima Zahra, Mohammed Jabari, et al. Prevalence of Anemia in a Population of Diabetics Casablanca Morocco. American Journal of Innovative Research and Applied 2019.
- Michalak Clinical Implications of the Coexistence of Anemia and Diabetes Mellitus in the Elderly Population. Journal of Diabetes Research. 2021; 8745968.
- Kabamba Tshikongo A, Kipenge Kyandabike R, Mwaba Mulubwa JJ, et al. Evaluation of the anemic condition of type 2 diabetes cases of the city of Lubumbashi. LA TUNISIE 2015; 93: 714-719.
- Larger, Anemia and Diabetes. Médecine des Maladies Métaboliques. 2021; 15: 570-571.
- Al Salman M. Anemia in Patients with Diabetes Mellitus Prevalence and General Med. 2015; 3: 162-165.
- Babitt JL, Lin Mechanisms of anemia in CKD. Journal of the American Society of Nephrology. 2012; 23: 1631-1634.
- Locatelli, F, Bárány P, Covic A, et Kidney disease Improving global outcomes guidelines on anemia management in chronic kidney disease a European Renal Best Practice position statement. Nephrology Dialysis Transplantation. 2013; 28: 1346-1359.
- Roger SD, McMahon LP, Clarkson A, et al. Effects of early and late intervention with epoetin alpha on left ventricular mass among patients with chronic kidney disease results of a randomized clinical trial. Journal of the American Society of 2004; 15: 148-156.
- Levin A, Li YC. Anemia and left ventricular hypertrophy in chronic kidney disease populations a review of the current state of Kidney International Supplements. 2002; S35-38.
- Makruasi, Nisa, Tanaya Siripoon, et Risk Factors Associated with Anemia in Type 2 Diabetes Mellitus with Moderate Renal Impairment. Journal of Hematology and Transfusion Medicine. 2022; 32.