The Brazilian National Immunization Program and Its Challenges for Modernization and Improvement
Author'(s): Ricardo Bordinhão*
BRL - Distribuidora de vacinas LTDA, Rio de Janeiro, RJ, Brasil.
*Correspondence:
Ricardo Bordinhão, BRL - Distribuidora de vacinas LTDA, Rio de Janeiro, RJ, Brasil, E-mail: bordinhao@brlvacinas.com.br.
Received: 27 January 2018; Accepted: 04 March 2018
Citation: Bordinhão R. The Brazilian National Immunization Program and Its Challenges for Modernization and Improvement. Clin Immunol Res. 2018; 2(1): 1-7.
Abstract
Although the decision making for vaccination strategies is done individually it is strongly influenced by social and public policies. Over the last few years, the Brazilian National Immunization Program (PNI) has registered a 95% rate of national vaccination coverage, which is similar to the rates observed in developed countries. The current challenges to be overcome by the program in order to preserve its excellence are to maintain its high rates of vaccination coverage, access equality, vaccination coverage monitoring, and safety, among others. The aim of the present work is to analyze the development of the PNI program over the last decades along with its challenges and prospects for modernization and improvement. The research methodology used in the present work was one of descriptive and bibliographical survey based on the Brazilian population data. The collection of data occurred between May and June of 2017 in the city of Rio de Janeiro - RJ - Brazil. Over the last years there has been a decrease in the rate of hospital admissions for the following diseases: measles, meningitis, tetanus, influenzas, pneumonia and others. Nevertheless, the access to information remains fragmented due to low informatization levels of the processes. The investments made in immunization generates countless benefits to the healthcare system and, consequently, to the health of the Brazilian population. Despite the high vaccination rates, the PNI program still needs improvements, especially in terms of modernization and informatization of the healthcare system. Nevertheless, its effective implementation demands investments for the acquisition and maintenance of new technologies, training of professionals, an organizational change, certification criteria and interoperability standards. Additionally, one of the main challenges for the PNI program is to align the strategies of verification and monitoring of disease risk perception and adverse events following vaccination (AEFV) among the different agents involved.
Keywords
Introduction
Alongside with human evolution, health treatments and assistance have been showing great breakthroughs throughout the years. The advances in technology and the good quality data collected by researchers have contributed with techniques, information, equipment and professionals capable of providing health assistance, immunization, treatments and highly complex surgical procedures.
On the other hand, the management of national health systems and services has always been the greatest challenge for governments in many parts of the world. In Brazil, the difficulties in providing primary healthcare to the population are being gradually overcome. However, despite the conquered improvements, actions are still strongly needed in order to maintain the advancements in the healthcare system.
Over the last few years, the Brazilian National Immunization Program (PNI) has registered a 95% rate of national vaccination coverage, which is similar to the rates observed in developed countries [1].
In general, Brazil has had great advancements in its healthcare system since the Federal Constitution of 1988. In this constitution health was granted to all the population as a right and was made an obligation of the state. This constitution also implemented the SUS – Unified Health System. From that moment on, healthcare services were decentralized and the new focus became to achieve equity, integrity and universality of the healthcare services. As of 1988, “the access to healthcare services became mandatory and free to all the Brazilian population” [own translation] (BRASIL, 2001 p. 53; MENDES, 1999 p. 135). With this, “health care was now tied to the life quality of the population, along with all the different social, cultural and economic features related with the causes of sickness of individuals and collectivities” [own translation] [2].
With regard to immunization, Brazil has the National Immunization Program (PNI), which was created in 1973 by the Ministry of Health and officially formalized under the Federal Law nº 6.259/1975. This law sought to systemize vaccination at a national scale and, therefore, improve the levels of immunization in the country [3]. Moreover, it addressed some challenges such as the reduction of morbidity and mortality caused by diseases that could now be fought against with immunization, which represented a major breakthrough for public health [4].
According to Júnior [1]:
“This change was fundamental to ensure the consistency of the vaccination schedule, the sustainable introduction of new vaccines, the technical standardization and the adoption of innovative strategies such as the combination of routine vaccination schedules with immunization campaigns, which played a decisive role in the eradication of poliomyelitis and measles achieved through the PNI”.
Although the PNI allows access to basic healthcare, there are still some challenges such as the maintenance and increase of vaccination coverage rates, access equality, monitoring of vaccination coverage, safety and others that must be faced and overcome so that the level of excellence of the program is preserved [5].
The aim of the present work is to analyze the development of the PNI program in Brazil over the last decades and also to analyze its prospects and future challenges for modernization and improvement. Furthermore, this work aims to evaluate the feasibility and necessity of informatization of the PNI system in the country.
This work is a response to the need for analysis and identification of issues, bottlenecks and demand for advancements that the National Immunization Program is currently facing in the country. Additionally, this work exposes the good results reached so far taking into account the great relevance of the program for the basic healthcare system and its access to a major portion of the Brazilian population.
Methodology
The present work was developed based on a bibliographical and qualitative research and the chosen methodology to be followed was the “descriptive research”. “In a descriptive research it is possible to develop a study, an analysis, a registration and interpretation of facts from the physical world without the interference of the researcher” [6].
A research can be defined as a systematic and rational investigation which aims to give answers to issues that are presented. “Researches are required when there is not enough information available to address an issue, or when the information available is in such a state of disorder that it cannot be properly related to the issue at hand” [7].
The present work was done in the city of Rio de Janeiro - RJ. However, its data were extracted from both scientific papers and books available digitally and from scientific papers and books available physically at public libraries of the city of Rio de Janeiro- RJ. The research was undertaken in the period from May 2017 to August 2017.
According to Gil [7], “through the analysis of the theoretical framework it is possible to have the necessary basis to understand the universe one intends to investigate”. The author also adds that this type of research is indicated when the goal of the research is to raise the level of familiarity with the issue and, thus, make it more explicit. Ultimately, the theoretical framework assembled provides the adequate basis to analyze and make conclusions about the data collected via the bibliographical research used to develop the present work and composed mainly of books and scientific papers.
In essence, by following this methodology this work aims to gather the necessary theoretical framework in order to provide a descriptive analysis, establish a historical organization of data about the topic and to make the analyzed data available to all the readers.
The Brazilian National Immunization System
Although the decision making for vaccination strategies is done individually it is strongly influenced by social and public policies. The immunization policy in Brazil is made of a system that aims to bring vaccination coverage to a larger amount of the target population. To reach this goal, there needs to be appropriate environmental conditions such as well-equipped vaccination rooms as well as a sufficient amount of vaccines and supplies to meet the demand of the Brazilian population [8].
In Brazil, there are currently five main health information systems within the Ministry of Health: the Mortality Information System (SIM), the Live Births Information System (SINASC), the Public Hospital Information System (SIH-SUS) and the Ambulatory Care Information System (SIA-SUS) [9].
With this in mind, not only is it important to understand vaccination as an essential part of basic healthcare as it promotes monitoring, prevention and protection of public health but also to highlight the fact that it is one of the main components of the Unified Health System (SUS) [8]. The PNI follows a routine immunization schedule but it also operates in wider ranges of activities. For example, it gives special attention to disease prevention and control during national vaccination campaigns that usually prioritize specific diseases at different times (MS, 2003). The routine immunization schedule takes the National Vaccination Schedule into consideration and, therefore, it promotes the vaccination of the population according to the schedule considered ideal by the Ministry of Health [10]. By doing so, the PNI guarantees mass immunization and interrupts disease transmission [10].
Regarding the National Vaccination Schedule, it can be observed that between the years 2005 and 2015, four ordinances were issued by the Ministry of Health with the purpose to alter and include new vaccines in the National Vaccination Schedule [11]. These ordinances were the following: Ordinance No. 1.602/2006; 1.946/2010; 3.318/2010 and 1.498/2013 [11].
As a result of the promulgation of each of these ordinances, the following nine vaccines were included in the National Vaccination Schedule: Hepatitis A (hepA), Meningococcal C Conjugate (Men-C), HPV, DTP, Rotavirus, 5-valent and 10-valent pneumococcal, MMR and inactivated polio vaccine (IPV). One of the reasons why these vaccines were included was due to the high occurrence rates of their respective vaccine-preventable diseases. Some other reasons were the aim to implement a precaution measure against the reintroduction of diseases already eradicated in the country, to introduce combination vaccines consisting of various antigens, among others [12].
Vaccines included in the National Vaccination Schedule
In this chapter there will be a brief presentation of the main types of vaccines included in the National Vaccination Schedule, in accordance with Aquino [12], in addition to some essential information about the disease or its causative agent, also in accordance with the cited authors found in Aquino [12].
Oral Vaccine against Rotavirus (VORH2)
2VORH stands for “Vacina Oral contra Rotavirus Humano” which literally translates to “Oral Vaccine against Human Rotavirus”
The rotavirus causes a severe type of diarrhea among infants. The rotavirus is the main causative agent of this type of diarrhea in a worldwide scale and it contaminates approximately 125 million people per year [13].
Ten-valent Pneumococcal Conjugate Vaccine
This vaccine aims to prevent invasive pneomococcal disease (IPD) such as bacteremic pneomococcal pneumonia, meningitis, sepsis and acute otitis media caused by Streptococcus pneumoniae [11]. “The Streptococcus pneumoniae is one of the main causative bacterium of infections in infants between 0 and 2 years old and it is also responsible for over 1.9 million deaths annually” [14].
Meningococcal C Conjugate (Men-C)
Meningitis can be caused by infection by bacteria, viruses and protozoa. “In 2009, 75% of the cases of meningococcal disease caused by Neisseria meningitidis were associated with the serogroup C, which makes vaccination the most efficient way of prevention against this disease” [15].
Inactivated Polio Vaccine (IPV)
Poliomyelitis is a highly contagious disease which mainly affects children under 5 years old. In a range from 1% to 2% of the cases, the disease causes permanent paralysis, usually in the lower limbs which is irreversible [12].
Pentacel Vaccine
Pentacel is a combination vaccine that gathers five immunizations in a single dose. It is recommended to improve immunity against diphteria, tetanus, pertussis, hepatitis B and Haemophilus influenzae type b [16].
MMR Vaccine
This vaccine substitutes the triple viral vaccine for 15 month old children. It prevents varicella in addition to preventing measles, mumps and rubella [8].
Hepatitis A Vaccine
This disease is common throughout the world, however, in countries where there are low sanitary and socioeconomic conditions there is a higher occurance of the disease [17].
Human Papillomavirus Vaccine (HPV)
The papillomavirus has oncogenic potential and it is responsible for over 70% of the cases of cervical cancer and for over 90% of anogenital lesions [18].
Diphtheria-tetanus-acellular Pertussis Vaccine (dTpa)
This vaccine is commonly recommended for pregnant women as reinforcement or as a complement for the Td vaccine (tetanus and diphtheria). This vaccine helps decrease the incidence rate of mortality caused by pertussis in newborns [11].
National Vaccination Schedule
The National Vaccination Schedule is composed with a series of legal instruments that establish the necessary supply of vaccines in accordance with the goals of the Brazilian National Immunization Program.
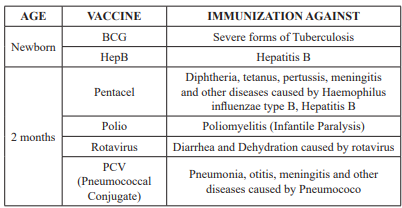
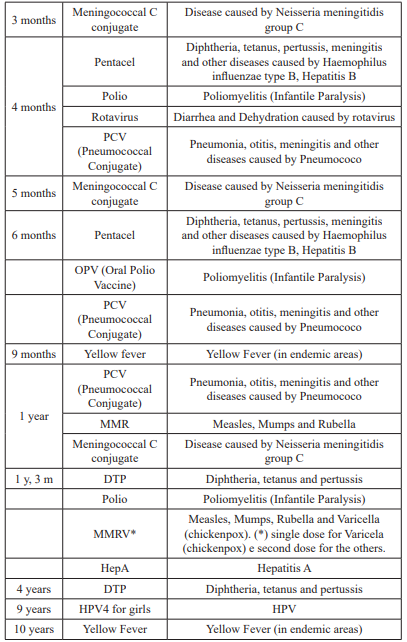
Table 1: National Vaccination Schedule of 2017 [28].
Nowadays, Fiocruz guarantees the supply of the essential vaccines for the Basic Vaccination Schedule of the Brazilian Ministry of Health [19]. Which leaves room for actions that aim at the improvement of quality and effectiveness of patient’s immunization, as well as the control of these processes, which tends to become a fully computerized system in the future.
The Immunization and the Results In Terms of Disease Prevention The investments made in immunization result in countless benefits to the healthcare system and, consequently, to the health care of the Brazilian population. Over the last years there has been a decrease in the number of hospital admissions for the following diseases: measles, meningitis, tetanus, flus, pneumonia, among others. However, the access to information is still fragmented due to the low informatization levels of the processes.
According to Junior [1], these are the numbers registered in regard to the main diseases treated with immunization in Brazil:
“In 2012, the polio vaccination campaign for children less than 5 years old reached coverage rate of 98.9% of the target audience although the disease had already been eradicated in the country. Other successful campaigns were the rubella campaign in 2008, which reached 67 million people and the pandemic influenza campaign in 2010, which reached 97 million people. The last campaign that aimed to maintain measles elimination, in 2011, reached 98.5% of the target audience and had 16.7 million children vaccinated between the ages 0 and 7. In the seasonal influenza campaigns the coverage rates reached in Brazil are considerably high in comparison to other countries. In 2011, a coverage rate of 86% of the target population was reached in the country”.
In Brazil not only was the eradication of poliomyelitis and variola achieved but also the elimination of the measles virus circulation since 2000 and the rubella virus since 2009 [19]. Additionally, a sharp decline was registered in the number of cases and incidence of Vaccine-Preventable Diseases such as meningococcal meningitis, diphtheria, neonatal tetanus, among others [19].
Official data from the Ministry of Health show that Brazil was the first country to introduce the vaccine against the rotavirus in the public healthcare system. Over 60% of the children under 1-year old were benefited in 2006, the first year of this implementation. In 2009, the percentage of the population immunized with two doses of the rotavirus vaccine reached the rate of 84.26% [18].
In a study undertaken about the Varicella disease, the authors Hirose et al., [20], concluded that the USA reduced the varicella-related hospitalization rate of children under 4 years old in 81,4%-99,2%, 6-14 years after the implementation of the universal vaccination against the disease (1995) reaching a vaccination coverage of 90%. In Uruguai, the hospitalization rates were reduced in 94% (1-4 years old) in 6 years, reaching a vaccination coverage of 90%; Canada: 93% of hospitalization reduction (1-4 years old) in 10 years, vaccination coverage of 93%; Germany: 62,4% of hospitalization reduction (1-4 years old) in 8 years, vaccination coverage of 78,2%; Australia: hospitalization reduction of 76,8% (1-4 years old) in 5 years, vaccination coverage of 90%; Spain: 83,5% of hospitalization reduction in 4 years, vaccination coverage of 77,2%; and Italy: reduction of 69,7%-73,8% (general population), vaccination coverage of 60%-95%.
In Brazil, the Ministry of Health estimates that since 2015 more than 45 thousand pneumonia-related hospitalizations were reduced yearly throughout the country. They also estimate that the average reduction of the pneumonia-related hospitalization was of approximately 83% [11].
Even though the National Immunization Program makes immunobiologicals available on a regular basis through the Vaccination Schedules free of cost for the population, social inequalities and differences in the use of these immunobiologicals can still be identified [21]. The promotion of educational activities and projects is also important as they can promote awareness about the importance of vaccination. The more awareness is promoted, the more the population will fully respect and adhere to the vaccination schedule, which will significantly reduce the incidence of Vaccine-Preventable Diseases [22].
The Need for Improvement and Informatization of the Health Information Systems
Despite the high vaccination coverage rates reached in Brazil, some improvements are still needed in the PNI especially regarding its modernization and system informatization. By meeting the demand for modernization and informatization of the PNI it will be possible to tackle the inequalities, improve and expand the immunization rates. As a final result, the users of the PNI would benefit in various ways.
According to Brasil, this perception gives special attention to the following items:
“(1) to the context of healthcare as an action of basic healthcare service; (2) to the commitment of incorporating new vaccines and new target audiences; (3) to the understanding that effective vaccination requires commitment with the efficiency and quality of the different components of this activity; (4) to the commitment with the investigation and analyses of the adverse events following vaccination; (5) to the investment in training of professionals involved; (6) to the continuous search for results that represent relevant impact in the context of vaccine-preventable diseases under surveillance”.
For an immunization policy to be adequate and realistic there must be a commitment of introducing new vaccines on a regular basis (including the reduction of injections) and the expansion in number of the target audiences [8].
The investments in technology already made by the Ministry of Health have clearly improved the immunization system; however, these improvements must be maintained and expanded. This way, the PNI can be consolidated once and for all as the main means of health care for the Brazilian population [8].
The PNI outcomes in terms of control over Vaccine-Preventable Diseases have put Brazil in the same level of outcome as of developing countries. This achievement was a result of the implementation of strategies that aimed at expanding vaccination coverage rates, public policies for immunobiologicals self- sufficiency besides initiatives focusing on the guarantee of safety through passive surveillance for AEFI - adverse events following immunization [23].
According to the authors ROSS et al., [24], the informatization of the healthcare system must be made together with different organizations and entities as well as with the intervention of public authorities to support and guide this process. These authors suggest the following five ideal scenarios for the creation and implementation of the informatization systems: “1) reorganize the data available of the main healthcare events as to facilitate the linkage between different databases; 2) set up Standards for the creation of integrated systems that would allow the participation of relatives, healthcare related organizations and Public Health agencies; 3) develop an integration policy for the current healthcare systems; 4) allow access to information for family; and 5) promote evaluation studies about the role of the information systems” [24].
Another interesting solution that should continue to be promoted is the implementation of electronic medical records. Because, “an electronic medical record available online would allow the patient to review, take notes or keep track of their health condition, including their vaccination status, which would create a communication bridge between the patient and the healthcare service providers” [23].
The integration of all the health information systems is essential to make this tool effective at providing adequate indication of special immunobiological vaccines for adults and children. If not, there is a great risk of patients being immunized twice with the same antidote by different healthcare entities [23].
Still on this topic, the authors Luhn amd Waldman [23], have concluded through a study undertaken in the USA that 22% of the investigated children had received vaccines in more than one entity, showing how the lack of an integrated database compromises the ability to identify the vaccination needs of the patients [23].
Furthermore, in other studies undertaken in the USA and Australia, it has been shown that the main contribution of the informatization of the healthcare systems was the increase in the vaccination coverage rates and its role as a tool of support for the recall/remind systems [23]. The greatest advantages of the informatization of the healthcare systems and the electronic medical records are the improved management and optimization of vaccines, the integration with other electronic databases, the notification of adverse events, the new registration features and the registered vaccination records over patients’ lifetimes [23].
According to Neves; Junges [25], it is extremely important that actions are promoted in favor of the improvement of the information systems. Actions such as:“the consolidation of data at both local unit and municipality level; a shift in the system in a way that it allows municipalities to incorporate modules according to their specific regional needs; higher connectivity and integration among the other information systems within the Unified Health System to avoid unnecessary overlapping of information within the systems; and to promote education and training for health professionals to raise their awareness about the importance of the SIS as a tool for epidemiological surveillance” [25].
Still according to Neves; Junges [25], it would be best to have a system in which the data was analyzed with the correspondent municipality. This way, the process would become more agile and efficient besides being an opportunity to receive subsidies to fund the planning and execution of healthcare related actions.
Similarly, the evaluation of the efficiency and duration of the immune response promoted by these new vaccines, as well as its safety, requires a long and thorough monitoring process [26].
That being said, one of the biggest challenges for the upcoming years is the expansion in the number of researches in biology, immunology and immunopathology of vaccine-preventable diseases in order to understand the causalities and pathogeny of the AEFI [26].
Equally important, the surveillance for vaccine-preventable diseases must give special attention to the analysis of the medium and long term impact of different vaccination strategies as well as of its risk/benefit effects [27].
Therefore, the development of this strategy, as long as it is implemented according to safety and confidentiality criteria, will make information systems user-friendly and functional, representing a historic breakthrough in the health care of the Brazilian population [23].
Final Considerations
The Brazilian National Immunization Program has been reaching excelent results in terms of vaccination coverage with similar rates to the ones registered in developed countries. Nevertheless, there is clear need for modernization, improvements and system informatization adjustments in the Program.
It is highly necessary that the healthcare systems of the different federative units become computerized and interconnected. However, implementing these changes demands investments for the acquisition and maintenance of the new technologies, training of professionals, an organizational change, certification criteria and interoperability standards.
Additionally, one of the main challenges for the PNI program is to align the strategies of verification and monitoring of disease risk perception and adverse events following vaccination (AEFV) among the different agents involved.
In the final analysis, the present work also highlights the need for further and deeper studies about the proposed theme. It is of great importance that further studies are developed and given exposure within the academic community as to provide guidance to any professionals who might feel interested about it.
References
- Junior BdaS. 40 anos do Programa Nacional de Imunizações uma conquista da Saúde Pública brasileira. Epidemiol. Serv. Saúde. 2013; 22: 1.
- Constituição de. Constituição da República Federativa do Brasil. Brasília. Senado. 1988.
- Barbieri CLA, Dias C, Santos MA. et al. Cobertura vacinal infantil em um service filantrópico de 40 atenção primária à saúde do Município de São Paulo, Estado de São Paulo, Brasil, em Epidemiologia e Serviços de Saúde, Brasília.2013; 22: 29-139.
- Pinto LLS. O programa nacional de imunizações para além do controle das doenças imunopreveníveis. Uma história de 30 anos. Revista Baiana de Saúde Pública. 2004; 28: 91-95.
- Sato APS. National Immunization Program: Computerized System as a tool for new challenges. Rev Saúde Pública. 2015; 49: 39.
- Barros AJdaS, Lehfeld Fundamentos de metodologia científica. 3. ed. São Paulo: Pearson Prentice Hall. 2007.
- Gil A C. Como Elaborar Projetos de Pesquisa. São Paulo: ATLAS. 2002.
- Brasil, Ministério da Saúde. Secretaria de Vigilância em Saúde. Departamento de Vigilância Epidemiológica. Programa Nacional de Imunizações PNI: 40 anos. Brasília Ministério da Saúde. 2013; 236.
- Barbosa Sistemas de informação em saúde a percepção e a avaliação dos profissionais diretamente envolvidos na atenção básica de Ribeirão Preto / SP. 2006. 100f. Dissertação Mestrado - Departamento de Medicina Social, USP, Ribeirão Preto. 2006.
- Moraes JC, Ribeiro MCSA, Simoes O, et Qual é a cobertura vacinal real Epidemiologia e Serviços de Saúde. 2003; 12: 147-153.
- http://www.brasil.gov.br/saude/2014/04/confira-asprincipais-acoes-do-programa-nacional-de-imunizacoes-1
- Aquino LMde. Programa Nacional de Imunizações: a evolução docalendário de vacinação por meio da implantação de novas vacinas nos últimos 10 Trabalho de Conclusão de Curso. 2016. Faculdade de Economia, Administração e Contabilidade da Universidade de Brasília. BRASÍLIA – DF. 2016.
- Miller MA, Mccann Policy analysis of the use of hepatitis B, Haemophilus influenzae type B-, Streptococcus pneumoniae- conjugate and rotavirus vaccines in national immunization schedules. Health Economics. 2000; 9: 19-35.
- Gouvea V, Santos N, Timenetsky MCST. Identification of bovine and porcine rotavirus G types by PCR. Journal of Clinical Microbiology, Washington. 1994. 32: 1338-1340.
- Brasil, Ministério da Saúde. Secretaria de Vigilância em Saúde. Departamento de Vigilância Epidemiológica. Coordenação Geral do Programa Nacional de Imunizações. Informe técnico introdução da vacina meningocócica C conjugada no Calendário de Vacinação da Criança. Brasília Ministério da Saúde. 2010; 47.
- Brasil, Ministério da Saúde. Secretaria de Vigilância em Saúde. Departamento de Vigilância Epidemiológica. Coordenação Geral do Programa Nacional de Imunizações. Informe técnico da introdução da vacina pentavalente – vacina adsorvida difteria, tétano, pertussis, hepatite B (recombinante) e Haemophilus influenzae tipo b conjugada. Brasília: Ministério da Saúde. 2012.
- Zachoval Rabb J, Zachoval V, Deinhardt F. Circulating interferon in patients with acute hepatitis A. Jounal of Infecious Diseases. Oxford. 1986; 153: 1174- 1175.
- Schiller JT, Lowy DR, Markowitz Human papillomavirus vaccines. In Plotkin, S.A. Orenstein, W. Offit, P.A. Vaccines. Elsevier Saunders. 2013; 234-256.
- Cobertura Vacinal: Referência no controle e eliminação de doenças. Revista RADIS. Disponível em. 2011.
- Hirose M, Gilio Ae, Ferronato AEF, et al. Impacto da vacina varicela nas taxas de internações relacionadas à varicela revisão de dados Rev. Paul Pediatr. 2016; 34: 359- 366.
- Barata RB, Pereira SM. Desigualdades sociais e a cobertura vacinal na cidade de Salvador, Bahia. Revista Brasileira de Epidemiologia. 2013; 16: 266-277.
- Barros MGM, Santos MCS, Bertolini RPT, et Perda de oportunidade de vacinação aspectos relacionados à atuação da atenção primária em Recife, Pernambuco, 2012. Epidemiologia e Serviços de Saúde, Brasília. 2015; 24: 701- 710.
- Luhmi KR, Waldman Sistemas informatizados de registro de imunização uma revisão com enfoque na saúde infantil. Epidemiol. Serv. Saúde. 2009; 18: 1.
- Ross DA, Hinman AR, Saarlas KN, et al. The Near-Term Future for Child Health Information Systems. Journal of Public Health Management Practice. 2004; 10: S99-S104.
- Neves FdeA, Junges Sistema de informação em saúde como instrumento de avaliação da saúde da população. 2011; 8.
- Ward BJ. Vaccine adverse events in the new millenium is there reason for concern Bull World Health 2000; 78: 205-215.
- Waldman EA, Luhm KR, Monteiro Samg, et Vigilância de eventos adversos pós vacinação e segurança de programas de imunização. Rev. Saúde Pública. 2011; 45.
- Carlini Calendário Nacional de Vacinação. 2013. Disponível em: Acesso em: 08 ago. 2017.