Value of the Rapid Immunochromatographic Test for Diagnostic Guidance in the Diagnosis of Pharyngo-Tonsillitis Caused by Group A Hemolytic Beta Streptococcus (Abhs) In Southern Benin
Author'(s): Pamphile Aguessy1 , Durand Dah-Nouvlessounon1 , Selma Gomez2 , Bernix B. Soglongbe1, Victorien Dougnon3, Haziz Sina1, Adolphe Adjanohoun4 and Lamine Baba-Moussa1*
1 Laboratory of Biology and Molecular Typing in Microbiology, Department of Biochemistry and Cell Biology, Faculty of Science and Technology, University of Abomey-Calavi, 05 BP 1604, Cotonou, Benin.
2 Laboratoire de Biochimie et de Biologie Moléculaire and National Sickle Cell Disease Center, Université d’AbomeyCalavi, 01 BP 526 Cotonou, Republic of Benin.
3 Research Unit in Applied Microbiology and Pharmacology of Natural Substances, Research Laboratory in Applied Biology, Polytechnic School of Abomey-Calavi, University of AbomeyCalavi, Cotonou BP 526, Benin.
4 Institut National des Recherches Agricoles du Bénin (INRAB), Cotonou 01 BP 284, Benin.
*Correspondence:
Lamine BABA-MOUSSA, Laboratory of Biology and Molecular Typing in Microbiology, Department of Biochemistry and Cell Biology, Faculty of Science and Technology, University of Abomey-Calavi, 05 BP 1604, Cotonou, Benin.
Received: 11 Sep 2023; Accepted: 19 Oct 2023; Published: 26 Oct 2023
Citation: Aguessy P, Dah-Nouvlessounon D, Gomez S, et al. Value of the Rapid Immunochromatographic Test for Diagnostic Guidance in the Diagnosis of Pharyngo-Tonsillitis Caused by Group A Hemolytic Beta Streptococcus (Abhs) In Southern Benin. Clin Immunol Res. 2023; 7(1): 1-5.
Abstract
Background: Group A beta-hemolytic streptococcus (ABHS) tonsillitis is an acute disease that is often benign but sometimes serious due to its locoregional and general complications. It is a frequent cause of consultation among general practitioners, ENT and paediatrics. The choice and interest of our work was motivated by the fact that one of the most important acute upper respiratory infections is tonsillitis with the risk of serious complications. This study aims to determine the sensitivity and specificity of RDOT in the diagnosis of ABHA tonsillitis in southern Benin.
Methods: This was a prospective analytical and descriptive study carried out at the Vallée de Grâce Medical Clinic (CM VG) and at the Padre Pio Humanitarian Health Center (CSVH), at the Laboratory of Biology and Molecular Typing in Microbiology / UAC, in Benin over 12 months (July 2, 2022 and June 31, 2023). It included patients diagnosed with tonsillitis. All the patients included underwent a RDOT and a cytobacteriological examination of the throat swab (Gold Standard). We studied the following variables: age, sex, months, clinical signs, cytobacteriological examination of the throat swab and TROD results.
Results: We recorded 272 tonsillitis cases. 60 cases of group A beta-hemolytic streptococcal (ABHS) tonsillitis are confirmed by bacterial culture. Group A beta-hemolytic streptococcal tonsillitis accounted for 22.06% of tonsillitis. 133 men (49%) and 139 women (51%) were registered. 32 men (53.33%) and 28 women (46.67%) had SBHA tonsillitis. The highest frequency of isolation of group A streptococcus was observed in the age group [0 to 5[years with 27 cases out of 60, i.e. a proportion of 45%. SBHA tonsillitis are more frequent in the months of December and August with the respective proportions of 16.67% and 10%. The SBHA TROD performed showed a Sensitivity of 95%, a Specificity of 94%, a positive predictive value of 92% and a negative predictive value of 98%.
Conclusion: Streptococcal etiology represents 22.06% of tonsillitis in Benin. Our results reinforce the interest of RDOT and especially cytobacteriological examination in the etiological diagnosis of tonsillitis.
Keywords
Introduction
Tonsillitis or tonsillitis is considered an inflammation of the palatine tonsils of infectious origin. Group A beta-hemolytic Streptococcus (ABHS) tonsillitis is an acute disease that is often benign but sometimes serious due to its locoregional and general complications. It is the leading cause of consultation among general practitioners, ENT and pediatricians [1,2]. Pharyngo-tonsillitis is usually caused by viruses or bacteria; but the bacterial etiology is formidable due to its potentially serious locoregional and/or general septic complications. Among the bacteria responsible for tonsillitis, group A beta-hemolytic Streptococcus (ABHS) is the first cause found. They constitute a public health problem, due to their frequency, their recurrence and their socio-professional and economic impact [3-6].
The diagnostic problem in pharyngo-tonsillitis is usually considered in a binary manner, the objective being to distinguish cases linked to ABHS from cases of viral origin [7,8]. The chosen diagnostic strategy must be sensitive because patients with a false- negative result risk developing complications, and it must be sufficiently specific because false-positive results risk leading to unnecessary antibiotic consumption, contributing to the emergence bacterial resistance and generating unnecessary health costs. The different means of diagnosing GAS pharyngitis are throat swab culture, clinical examination and the rapid diagnostic orientation test (TROD) [9-12]. Tonsillitis has been the subject of little work in Benin. It is in this context that we decided to evaluate the sensitivity and specificity of TROD in the diagnosis of tonsillitis caused by group A beta-hemolytic Streptococcus.
Material and Methods
Study centers
The study was carried out in three centers: The Vallée de Grace Medical Clinic, the Padre Pio Humanitarian Health Center (CSVH) and the Laboratory of Biology and Molecular Typing in Microbiology.
Vallée de Grâce Medical Clinic (CMVG)
It is located in the Aidignon district, district of Togba, in the commune of Abomey Calavi, in the department of Atlantique in Benin. It is organized into several sections: reception, pharmacy, consultation rooms, hospitalization rooms, room, Maternity department, pediatric department, otorhinolaryngology and the laboratory. The laboratory has several units including: Bacteriology/ Parasitology, Serology, Biochemistry and Immunology.Padre Pio Humanitarian Health Center (CSVH)
The CSVH Padre Pio is located in the 6th arrondissement of Cotonou in the Akpakpa Dodomè district, Coastal Department. It is organized into several sections: reception, pharmacy, consultation rooms, hospitalization rooms, treatment room, sampling room, the Hepato-gastroenterology service, the pediatric services, Medicine, endocrinology, maternity, cardiology, obstetrics and gynecology,otolaryngology (ENT) and the laboratory. The laboratory also has several units including: Bacteriology/Parasitology, Serology, Biochemistry and Immunology.
Laboratory of Biology and Molecular Typing in Microbiology
Located in the Department of Biochemistry and Cellular Biology of the Faculty of Science and Technology of the University of Abomey-Calavi, it is a research laboratory in Microbiology (clinical and food), Biochemistry, Molecular Biology and pharmacology of natural substances.
Methods
Prospective analytical and descriptive study was carried out during 12 months (from July 2, 2022 to June 31, 2023).
Sampling and Variables analyzed
The patients who were sampled are those in whom the diagnosis of pharyngo-tonsillitis was made in the ENT and pediatric departments of the sturdy health centers on the clinical arguments (fever, odynophagia dysphagia, hypertrophy and redness palatine tonsils and pharyngeal inflammatory signs, earache, and digestive signs). Variables such as age, sex, month, clinical signs, sensibility and specificity of RDOT were studied.
Rapid Immunochromatographic Diagnostic Orientation Test (TROD)
This is an immune reaction which brings into contact the anti- streptococcus antibody carried by the TROD and the surface antigen of the Beta Hemolytic Streptococcus A (SBHA) carried by the sample. Two throat samples were taken directly from the tonsils by swab. The swab was then introduced and dipped into a test tube containing a mixture of 3 drops of reagent I and 3 drops of reagent II. After 1 minute, the swabs were removed and the test strip inserted for 5 to 10 minutes. The reaction is positive when two red lines appear on the strip and the patient is diagnosed with SBHA bacterial angina. It is negative when visualizing a single red line. For cytobacteriological examination, culture of the samples was carried out on fresh blood agar for streptococci.
Ethical aspects This research protocol was approved by the Scientific Ethics Committee of the Doctoral School (Life Sciences) of the University of Abomey Calavi (UAC), Benin under number UAC/FAST/EDSV/1562003 in accordance with national and local regulations. Likewise, all patients or their first-degree parents gave informed consent by verbal or written agreement and confidentiality was respected.
Data processing and analysis
Microsoft Excel 2019 spreadsheet was used for data processing and then subjected to a univariate or multivariate analysis of variance (ANOVA) using STATA 3 version 11.0 software.
Results
Patients sociodemographic characteristics
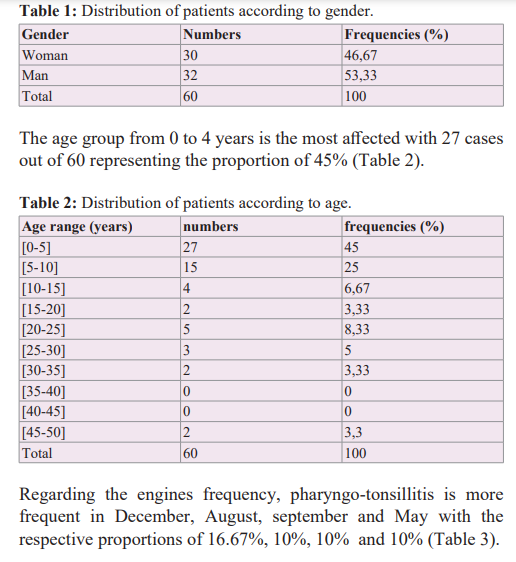
We recorded 272 cases of tonsillitis, 60 cases were positive for TROD and ECB from the throat swab. Average rate of 53.33 % are men compared to 46.67% women (Table 1) with a sex ratio of 1.14 in favor of the male sex. They belonged to age bracket from 3 months and 48 years with 11.20 ± 4 years as average age.
Discussion
Tonsillitis constitutes one of the main reasons for consultations in pediatrics and ENT in the health centers serving as the framework for the study with a prevalence of 9.39% and a bacterial proportion of 52.57%. SBHA tonsillitis has a prevalence of 22.06% and represents 41.95% of bacterial tonsillitis. Our prevalence of 22.06% agrees with the literature in which SBHA is present in 25 to 40% of acute tonsillitis in children and 10 to 25% of acute tonsillitis in adults [13]. Njifou Njimah et al. [14] in Mbouda found a prevalence of 9.84% with a proportion of 66.67% for bacterial tonsillitis. A prevalence of 7.53% among children aged 0 to 15 was found by Chobli et al. [15] in Cotonou. Gehanno et al. found a proportion of 38% for bacterial tonsillitis in France. From our study, it appears that the bacterial proportion of tonsillitis is higher as in the studies of Njifou Njimah et al. [14] in Mbouda, 66.67%; from Haidara et al. [16,17] in Dakar, 52.35% and from our compatriot Chobli et al. [15] in Cotonou 44.59%. The classic heat of tropical regions like ours favors the development of bacteria.
Njifou Njimah et al. [14], and Arama [18] reported that SBHA tonsillitis represent respectively 45% and 43% of bacterial tonsillitis while Chobli et al. [15] in Cotonou found a proportion of 24% for the SBHA. Our results corroborate with those of Njifou Njimah et al. [14] and Amara but superior to those of Chobli et [15]. The average age of 11 years found is lower than those of Njifou Njimah et al. [14] and Haidara et al. [17], which were 22 years and 26 years respectively. The extreme ages were 3 months to 48 years compared to 2 and 63 years for Njifou Njimah et al.and 1 to 72 years for Shaikh et al. [19]. The most represented age group [0-5[ corresponds to that of Chobli et al. [15] and is different from 10 to 19 years found by Njifou Njimah et al. [14] and Timbo et al. [20]. The sex ratio was 1, therefore absence of predominance of one sex, against the sex ratio is 1.14 and male predominance for Njifou Njimah et [14] and a sex ratio of 1.09 with a predominance masculine for Chobli et al. [15]. This lack of gender predominance could be due to the small size of the sample.
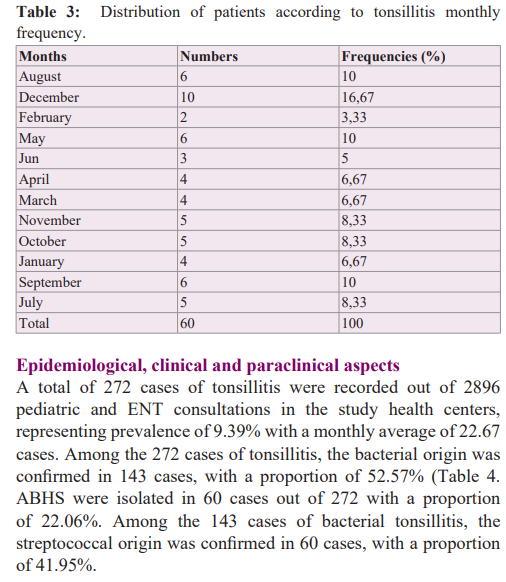
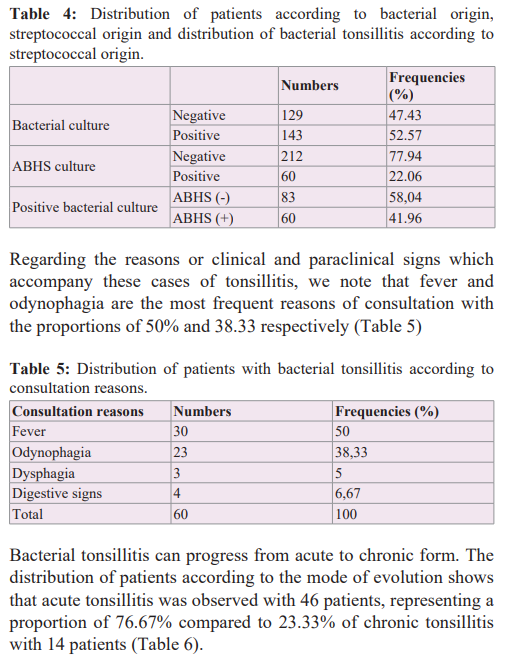
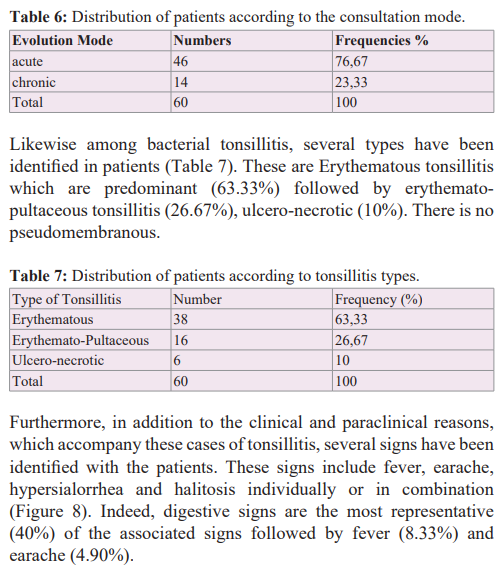
Acute tonsillitis was common (76.67%), this frequency is close to that of Njifou Njimah et al. [14] and Cohen et al. [21], who found 80% and 75% of acute forms respectively. This frequency is higher than that of Chobli et al. [15] who found 45.99% of acute tonsillitis. Fever and odynophagia were the most frequent reasons for consultation with the proportions of 50% and 38.33% respectively. The proportion 38.33% for and odynophagia is close to the 31.88% found by Chobli et al. [15] and lower than the 100% of Njifou Njimah et al. [14]. Erythematous tonsillitis (63.33%) were predominant, followed by erythematous-pultaceous (26.67%). Chobli et al. [15] found 12.02% of erythematous tonsillitis and 33.44% of erythematous-pultaceous tonsillitis in children aged 0 to 15 years. In our study, we also observed these predominances with a proportion significantly higher than that of Chobli et al.for erythematous tonsillitis and close to that of erythemato- pultaceous tonsillitis.
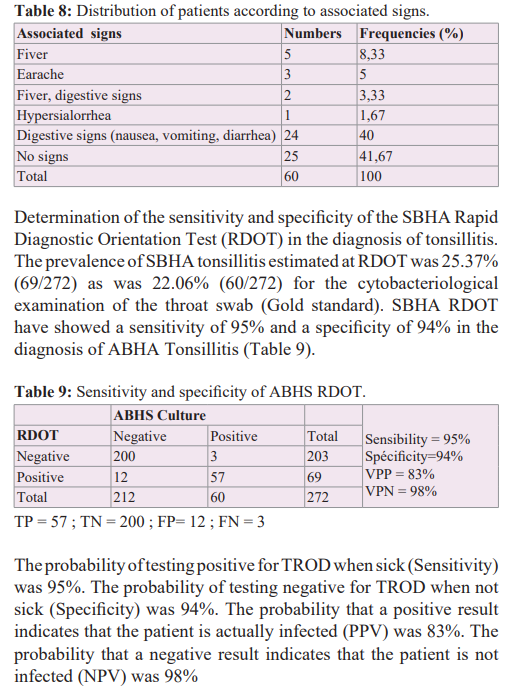
In our study, the prevalence of SBHA tonsillitis estimated with the Rapid Diagnostic Orientation Test (TROD) was 25.36% or 69 patients out of 272. This prevalence is lower than the 44.33% reported by Bola Siafa et al. [22] in Yaoundé, Cameroon. We noted that TROD was unable to identify 3 patients who were positive for SBHA culture (false negatives) and overestimated the diagnosis in 12 patients (false positives). In our study, we found a sensitivity of 95% and a specificity of 94% in the diagnosis of SBHA tonsillitis with 5% false negatives and 6% false positives. A positive predictive value of 83% and a negative predictive value 98% were found. Mezghani Maalej et al [23], reported a sensitivity of 93.2% and a specificity of 95.3% for the rapid diagnostic test compared to the reference method which is bacterial culture in Sfax in Tunisia. Our results are therefore similar to those obtained by Mezghani Maalej et al. in Tunisia. Bola Siafa et al. reported a RDOT sensitivity of 90.48%; a specificity of 90.90%. These figures are less good than ours in terms of validity for therapeutic care. In a study carried out by Rimoin et al. [24] in four developing countries, sensitivity ranged from 72.4% to 91% and specificity from 85.7% to 96.4%. These data are compatible with ours since the tests used are different.
The diagnostic problem in tonsillitis is usually considered in a binary manner, the objective being to distinguish cases linked to SBHA from cases of viral origin. The chosen diagnostic strategy must be sufficiently sensitive because patients with a false-negative result risk developing complications, and it must be sufficiently specific because false-positive results risk leading to unnecessary consumption of antibiotics, contributing to the emergence of bacterial resistance and generating unnecessary health costs. The practitioner is therefore confronted on a daily basis with a double dilemma: the microbial nature of acute tonsillitis (viral or bacterial) and the decision for antibiotic therapy (validation, type of antibiotic and methods of administration). In view of the sensitivity and specificity obtained in our study among the different diagnostic means of ABHS tonsillitis, the rapid diagnostic orientation test (RDOT) or the cytobacteriological examination of throat swabs are essential for an adequate prescription of antibiotic therapy in our growing antibiotic resistance.
Conclusion
Streptococcal etiology represents 22.06% of tonsillitis in Benin with strong resistance to erythromycin. Our results reinforce etiological research by RDOT and cytobacteriological examination of throat swabs with a view to limiting the selection of multi- resistant strains and ensuring effective and efficient treat.
Acknowledgement
We thank the patients and all others persons encountered during this study for their openness and collaboration
References
- Bidet P, Bonacorsi Facteurs de pathogénicité de Streptococcus pyogenes. Archives de pédiatrie. 2014; 21: S54-S61.
- Ferrie Questce quune angine Définition et signes cliniques de langine selon les Médecins généralistes et les internes de médecine générale de MidiPyrénées. thèse doctorat en médecine. 2017; 82.
- Maladies du nez de la cavité nasale et les sinus paranasaux le manuel pratique pour les étudiants de médecine générale de la spécialité Otorhinolaryngologie comp TI Karaseva. Universitéd Etat de médecine de Riazan. 2021; 72.
- Maizia A, Letrilliart L, Colin C, et Stratégies de diagnostic de langine aiguë en France une étude coûtefficacité. Presse Médicale. 2012; 41: 195-203.
- Bingen Résistance du streptocoque du groupe A aux macrolides. J Pediatr Puericult. 2005; 18: 349-353.
- Linda Évaluation des actesd amygdalectomie A lamygdalotome Service évaluation des actes professionnels. Haute Autorité de santé. 2006. www.has-sante.fr.
- Centor RM, Witherspoon JM, Dalton HP, et The diagnosis of strep throat in adults in the emergency room. Med Decis Making. 1981; 1: 239-246.
- Barry B, Lariven S. Manifestations systémiques au cours des infections pharyngées Encycl Méd Oto rhinolaryngologie. 2001; 20: 7.
- Agence Française de Sécurité Sanitaire des Produits de Santé Angine aiguë. Med Mal Infect. 1999; 29: 227-236.
- David R, Antibiotic Prescribing by Primary Care Physicians for Children with Upper Respiratory Tract Infections. Arch Pediatr Adolesc Med. 2002; 11: 1114-1119.
- Portier H, Peyramond D, Boucot I, et Évaluation de lapplicabilité du consensus sur la prise en charge de langine chez ladulte. Med Mal Infect. 2001; 31: 388-395.
- Shaikh N, Leonard E, Martin Jm, et Prevalence of streptococcal pharyngitis and streptococcal carriage in children A meta analysis. Pediatrics. 2010; 126: e557-e564.
- Wainsten Larousse medical 5e Ed Paris. Larousse. 2009; 52.
- Njifou Njimah. Thèse de doctorat en médecine Les Angines Bactériennes à Mbouda Epidémiologie Clinique et Health Sci. 2020; 21: 72-75.
- Chobli M, Yehouessi Vignikin B, Zoumenou E, et Prise en charge des angines de lenfant au CNHU de Cotonou. RAMUR. 2012; 17: 1.
- Le point actuel sur lépidémiologie des angines aiguës et des syndromes post streptococciques. Rev Prat. 1992; 42: 284-287.
- Haidara Les amygdalites et leurs complications aspect épidémiologique clinique et thérapeutique Thèse de doctorat en médecine Université des sciences des techniques des technologies de Bamako. 2014; 16.
- Arama A. Prévalence du streptocoque beta hémolytique du groupe A chez les enfants de 5 a 15 ans dans le service de ORL de lhôpital Gabriel Touré Thèse de doctorat en médecine Université des sciences des techniques des technologies de 2005.
- Shaikh JMN, Leonard Prevalence of streptoccal pharyngitis and streptococcal carriage in children a meta analysis. Pediatrics. 2010; 126: 557-564
- Timbo SK, Keita MA, Togola FK, et Aspects épidémiologiques de langine à Bamako. Mali Med. 2006; 4.
- Cohen Angine de lenfant. Rev Prat. 2007; 57: 1777-1783.
- Bola Évaluation du test de diagnostic rapide du streptocoque beta hémolytique du groupe A dans le diagnostic des angines. Health Sci. 2016; 17. www.hsd-fmsb.org.
- Mezghani Les angines aiguës de lenfant dans la région de Sfax épidémiologie et intérêt du test de diagnostic rapide. Médecine et Maladies Infectieuses. 2010; 40: 226-231.
- Rimoin AW, Fischer Walker CL, Hamza HS, et The utility of rapid antigen detection testing for the diagnosis of streptococcal pharyngitis in low resource settings. Int J Infect Dis. 2010; 14: 1048-1053.